
The quiet conclusion of a multi-billion pound digital funding wave has triggered something far more dramatic than policymakers expected. Across England’s hospitals, the market for electronic patient record systems is shifting from expansion to survival. Vendors that once chased growth are now fighting for position in a shrinking battlefield. Contracts being awarded today may lock suppliers into place for a decade. For those left outside the gates, the consequences could be existential.
For nearly four years, England’s hospitals experienced a rare surge of digital investment. Billions flowed into modernising infrastructure, accelerating the rollout of electronic patient records across the NHS. For vendors, it was a period of remarkable opportunity. Systems that had long struggled with fragmented technology suddenly had capital to replace legacy software and standardise clinical information. Trusts rushed to procure platforms capable of digitising entire hospital operations, from emergency departments to oncology pathways.
That moment is now ending. The funding programme that fuelled the rapid expansion of hospital record systems is closing its chapter. What follows will look very different. The next wave of productivity investment carries significantly less funding for core record systems. At the same time, procurement rules are tightening. Hospitals will no longer be able to quietly extend long standing technology contracts with the same ease that once defined the NHS digital market.
The result is a dramatic shift in behaviour among technology suppliers. Companies that previously relied on gradual contract extensions now face a far harsher reality. If they fail to secure a new deal in the next cycle, they could be locked out of the NHS acute hospital market for close to a decade. Hospital systems rarely change their core record platforms quickly once deployed. The switching cost is enormous. Entire clinical workflows, research systems, and operational processes become embedded within a single vendor’s architecture.
This reality has turned procurement into a high stakes contest. Vendors are scrutinising each tender with legal precision. Complaints over procurement decisions are becoming more common. Suppliers that once hesitated to challenge the NHS publicly are beginning to take a different view. When the alternative is exclusion from one of the world’s largest healthcare systems for ten years, reputational caution starts to fade.
There is also a deeper shift underway. For two decades, electronic patient record platforms have been the centrepiece of hospital digitisation. But the next phase of healthcare technology will be defined less by records and more by intelligence. The data stored inside these platforms is becoming the most valuable asset in modern medicine. Whoever controls access to those data environments holds the keys to training the next generation of clinical AI systems.
This explains the sudden intensity surrounding EPR procurement. Winning a hospital contract today does not simply mean selling software licences. It means securing the underlying data infrastructure for predictive analytics, automation, and machine learning tools that will reshape healthcare operations over the next twenty years.
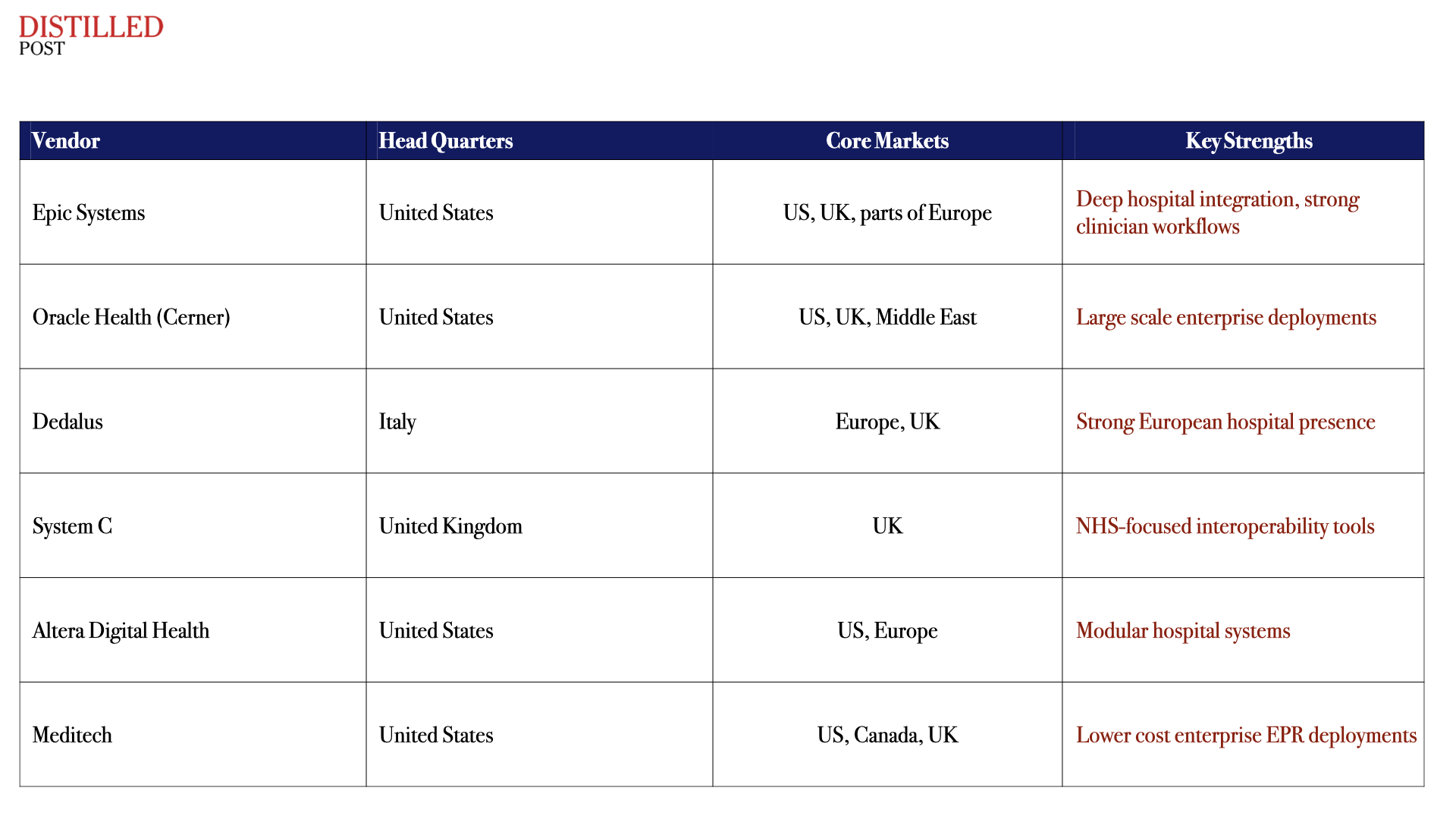
The United States presents a stark contrast. There, the market consolidated years ago around a handful of dominant platforms, with Epic emerging as the undisputed leader among major academic hospitals. Europe, by comparison, remains fragmented. Multiple regional vendors operate across different countries, often reflecting national healthcare structures.
England sits somewhere between those two models. The NHS historically supported a diverse vendor ecosystem. But the recent wave of large trust procurements has begun to tilt the market toward fewer, larger platforms. Several of the country’s biggest hospital groups have now standardised around a small cluster of systems capable of supporting complex multi site organisations.
The next decade will determine whether the NHS ultimately follows the American path of consolidation or retains a broader vendor mix. Much will depend on how hospitals prioritise interoperability and data access alongside clinical functionality.
One thing is already clear. The era when electronic patient records were simply an IT procurement exercise is over. These systems have become the digital backbone of healthcare itself. The companies that secure contracts today are not just selling software to hospitals. They are shaping the architecture through which future medicine will operate.
That is why the competition has become so fierce.
In the NHS technology economy, the next round of contracts will not simply decide who supplies software. They will decide who controls the operating system of British healthcare for the next generation.







