

There is a particular kind of governing failure that arrives not with a bang but with a series of quiet retreats. A policy is sound, the evidence is solid, the need is urgent. Then the polls tighten. A few activists grow restless. A rival party scents opportunity. And gradually, through procedural delays and strategic silences, something genuinely important gets quietly strangled. The NHS Federated Data Platform is at risk of exactly this fate.
The contract awarded to Palantir to build and operate the FDP has never been straightforward politics. The involvement of a US defence-adjacent technology firm in health data infrastructure carries a symbolic weight that is difficult to argue away, regardless of the contractual safeguards in place. Critics have latched onto that symbolism with understandable effectiveness. But the political environment surrounding the programme is now shifting in ways that go beyond reasoned scrutiny. With Labour facing potentially significant losses in the London local elections, including councils it has held for years across inner and outer boroughs, the temptation to appease sceptical voters by distancing itself from the FDP is growing. That would be a serious mistake.
The core case for the FDP rests on a structural problem that has persisted in the NHS for decades. Patient data sits in fragmented, incompatible systems across hundreds of trusts. A clinician treating a patient for a cardiac episode may have no visibility of that patient's oncology history held three miles away at a different hospital. Discharge planning is routinely hampered because social care records and acute hospital records exist in entirely separate administrative worlds. The inefficiency this creates is not abstract. It translates into delayed diagnoses, prolonged inpatient stays, duplicated tests, and a chronic inability to match resource deployment to patient need at the system level. The FDP is a practical response to that failure, designed to create the kind of integrated operational picture that modern healthcare management requires. No serious analyst of NHS infrastructure disputes that a solution to this fragmentation is necessary. The disagreement is about how to get there, and with whom.
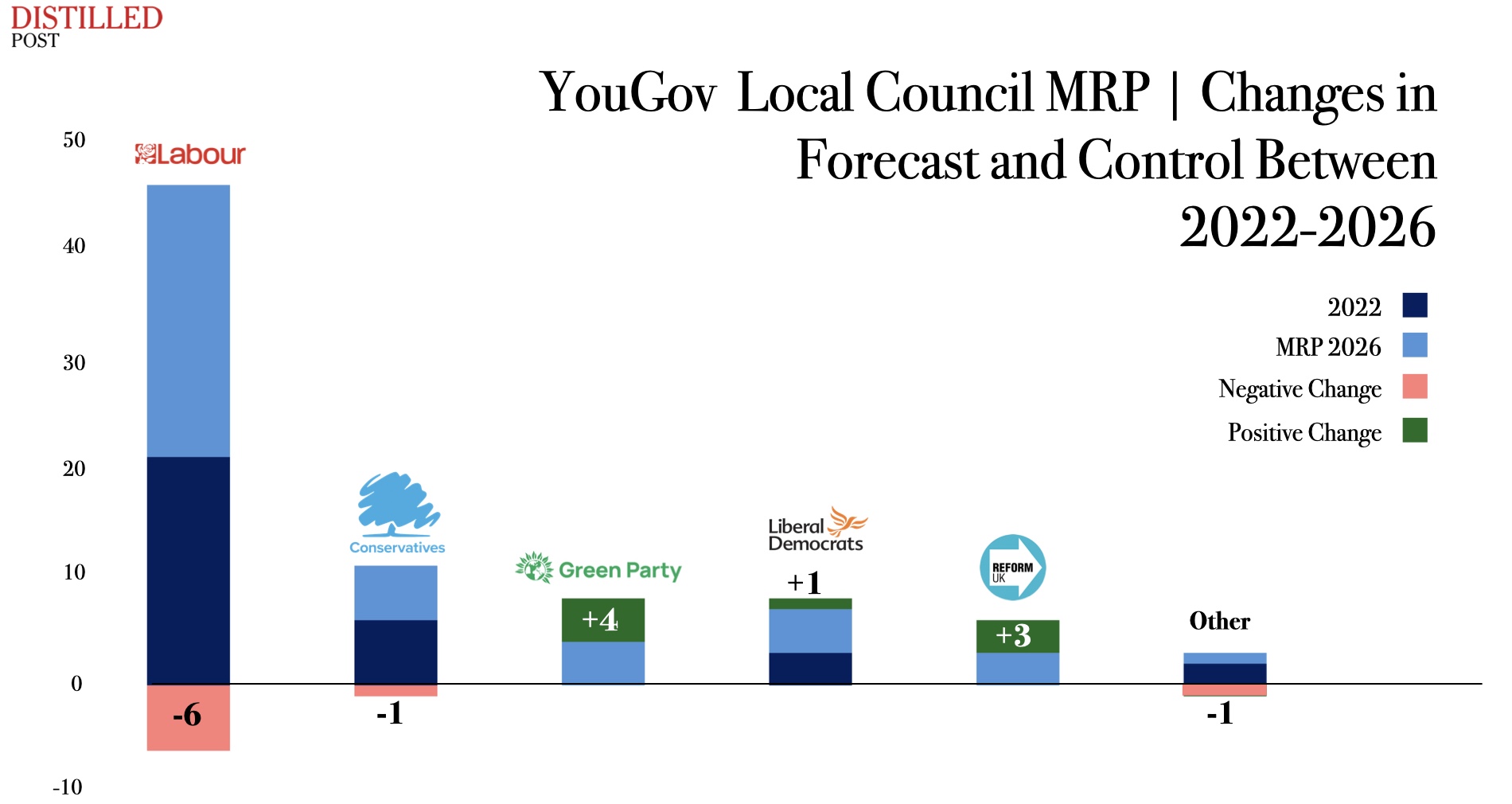
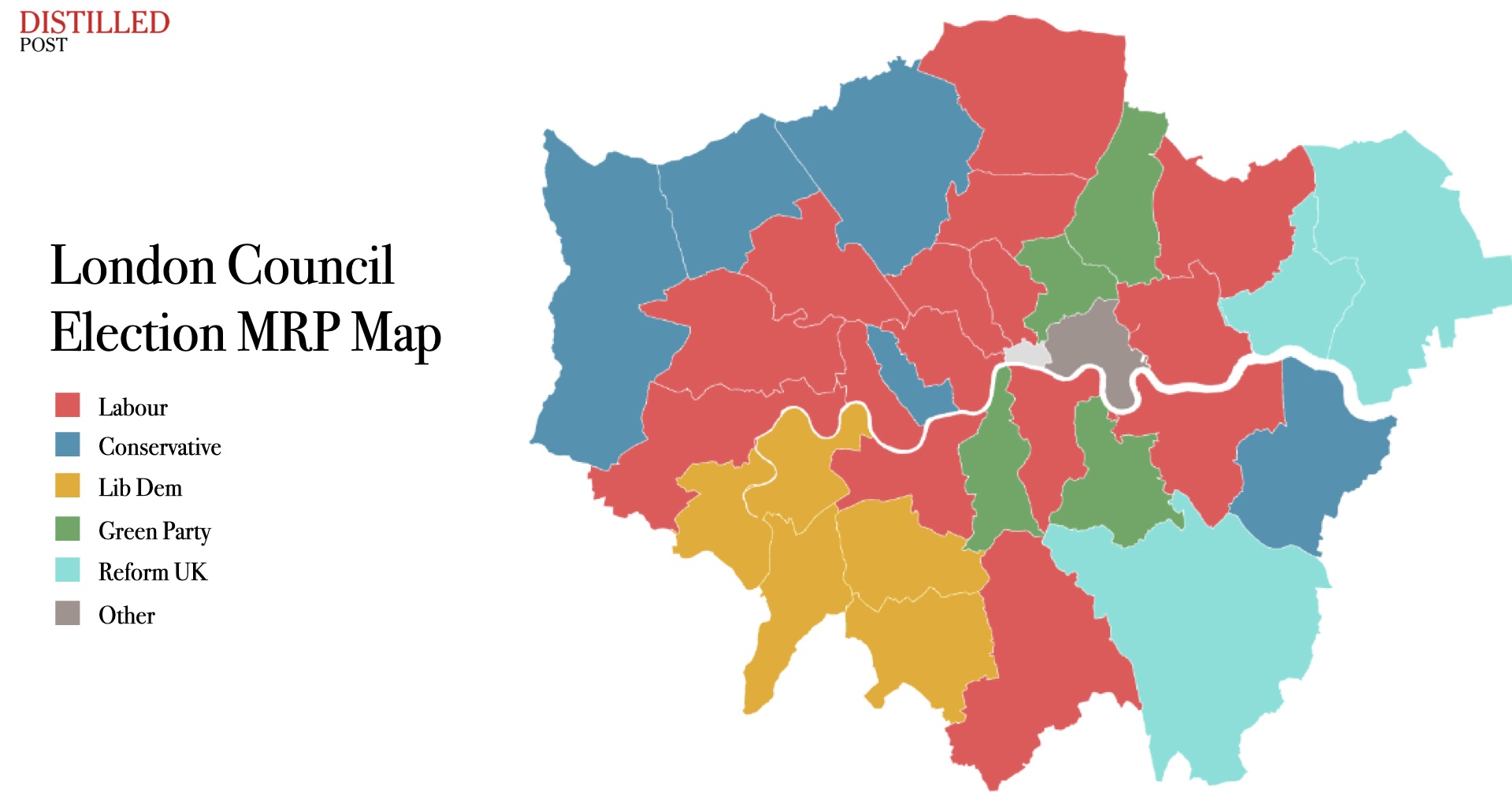
Into that disagreement have stepped the Greens and Liberal Democrats, deploying the FDP as a wedge issue in precisely the London constituencies where Labour's margin is thinnest. In boroughs like Hackney, Lambeth, and Lewisham, where progressive voters hold real expectations of their council administrations, the rhetoric of data sovereignty and corporate accountability lands with genuine force. The suggestion that a US firm with defence contracts should hold sensitive NHS data is rhetorically potent, even where the technical reality is more complicated. Palantir operates the platform; it does not own the data. The contractual architecture includes provisions that prevent secondary commercial use. These distinctions matter, but they do not make for compelling local campaign literature.
The Reform surge in outer London adds a further complication. Where Reform advances, Labour is forced into a defensive electoral posture that prioritises reassurance over governance. Councillors in Barnet, Havering, and Hillingdon are not primarily focused on the architecture of NHS data infrastructure. They are focused on visible local services, housing, and whether their voters feel economically secure. The national contract with Palantir barely registers as a local concern, except where campaigners make it one. But the aggregate effect of fighting elections on multiple fronts simultaneously is a leadership that becomes risk-averse, reluctant to defend positions that require sustained technical explanation, and increasingly inclined to postpone difficult decisions until the electoral weather improves.
The health service cannot operate on that timeline. Every month of delay in achieving meaningful data integration carries a clinical cost. Cancer referral pathways that depend on joining primary care, imaging, and pathology records across systems remain slower than they need to be. Elective recovery planning, which requires visibility of theatre capacity, staffing availability, and patient readiness across networks of trusts, remains partially blind. These are not hypothetical benefits being dangled by a technology firm seeking to justify its contract. They are operational necessities identified by NHS England's own clinical leadership. The political noise around the FDP should not be allowed to drown out the medical logic beneath it.
There is also a sovereignty argument being made by the wrong people for the wrong reasons. The concern about US corporate access to British health data is legitimate in principle. The question is whether the response to that concern should be to abandon integrated data infrastructure entirely, or to build the governance frameworks that make safe, accountable integration possible. True health data sovereignty is only achievable when the NHS has a functioning, coherent data architecture of its own. A system that remains fragmented is not sovereign; it is simply opaque, and opacity is not the same as protection.
The government's best defence against the political pressure it now faces is not to retreat from the programme but to be more specific and more disciplined about demonstrating what it delivers. The FDP rollout has proceeded across a number of trusts, and there is clinical evidence emerging about its operational effects. That evidence needs to be communicated with more precision, directly to local clinical audiences, and in terms that connect the platform's function to patient outcomes that people actually recognise. The ambiguity that has surrounded the programme's public communications has left a vacuum that critics have filled with more emotionally coherent narratives.






.jpg)
.jpg)