

NHS England has quietly placed nine hospital trusts into a new national turnaround programme designed for the system’s most troubled organisations. The move signals growing concern inside NHSE about persistent operational failure, financial pressure and leadership capability across major providers. Although framed as support, the intervention represents one of the strongest oversight tools the national body can deploy short of direct takeover.
For the organisations involved, the message from NHSE is clear. Improvement must accelerate rapidly or deeper structural action could follow.
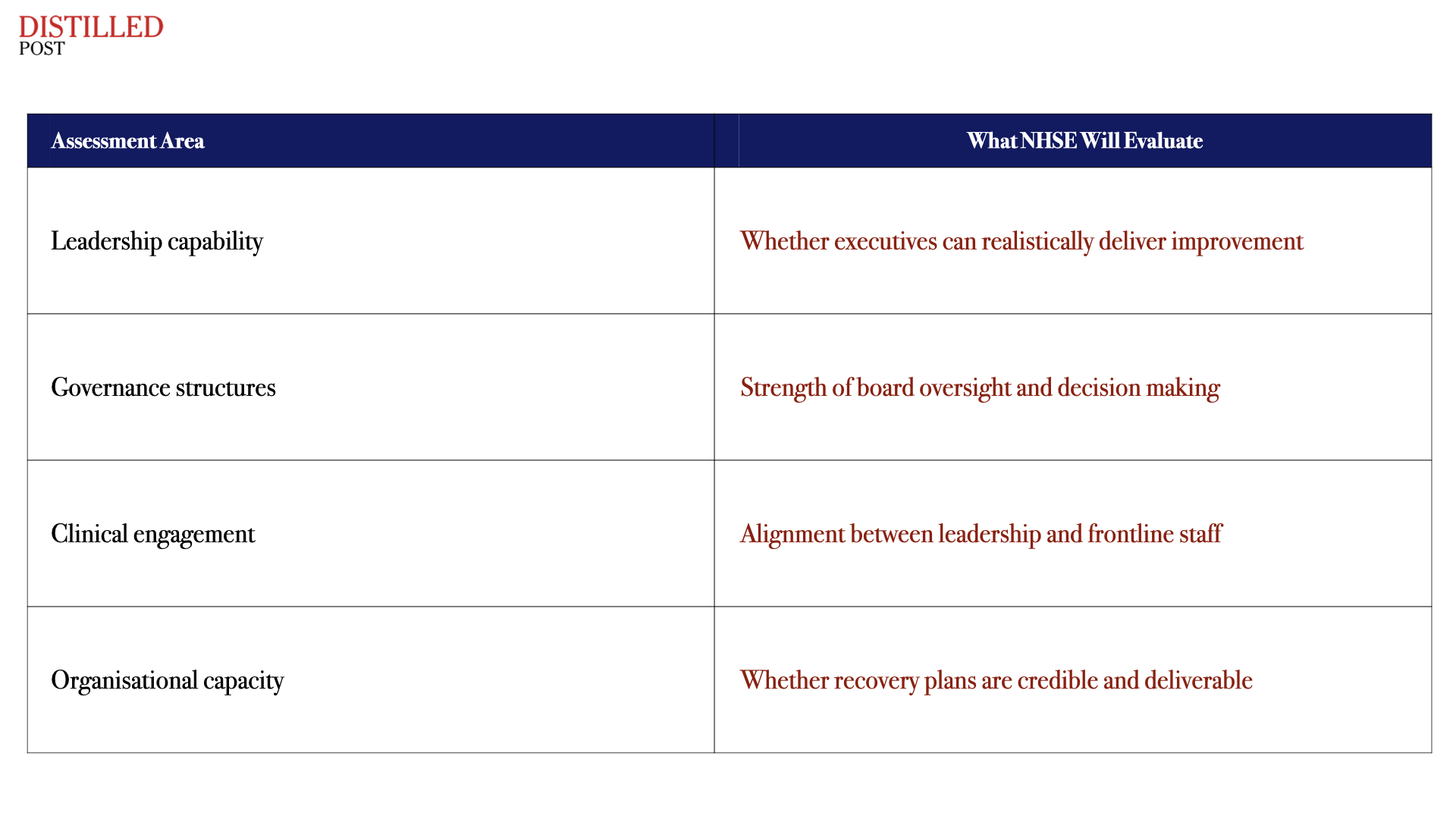
The new National Provider Improvement Programme marks a shift in how NHSE intends to deal with failing providers. Instead of relying solely on the traditional recovery frameworks used in recent years, the programme introduces a far deeper assessment of whether a trust has the organisational capability to recover at all. Over the next six to nine months NHSE teams will examine leadership quality, governance discipline, clinical engagement and operational planning across each organisation.
The process will not simply review performance metrics but will test whether the organisations possess the internal conditions required to deliver sustainable improvement. If NHSE determines that those foundations are weak, the programme may lead to leadership changes, tighter regulatory oversight or structural adjustments to how services are delivered across regional health systems. In effect, NHSE is asking a fundamental question about each provider.
Can the organisation fix itself or does the system need to intervene more directly.
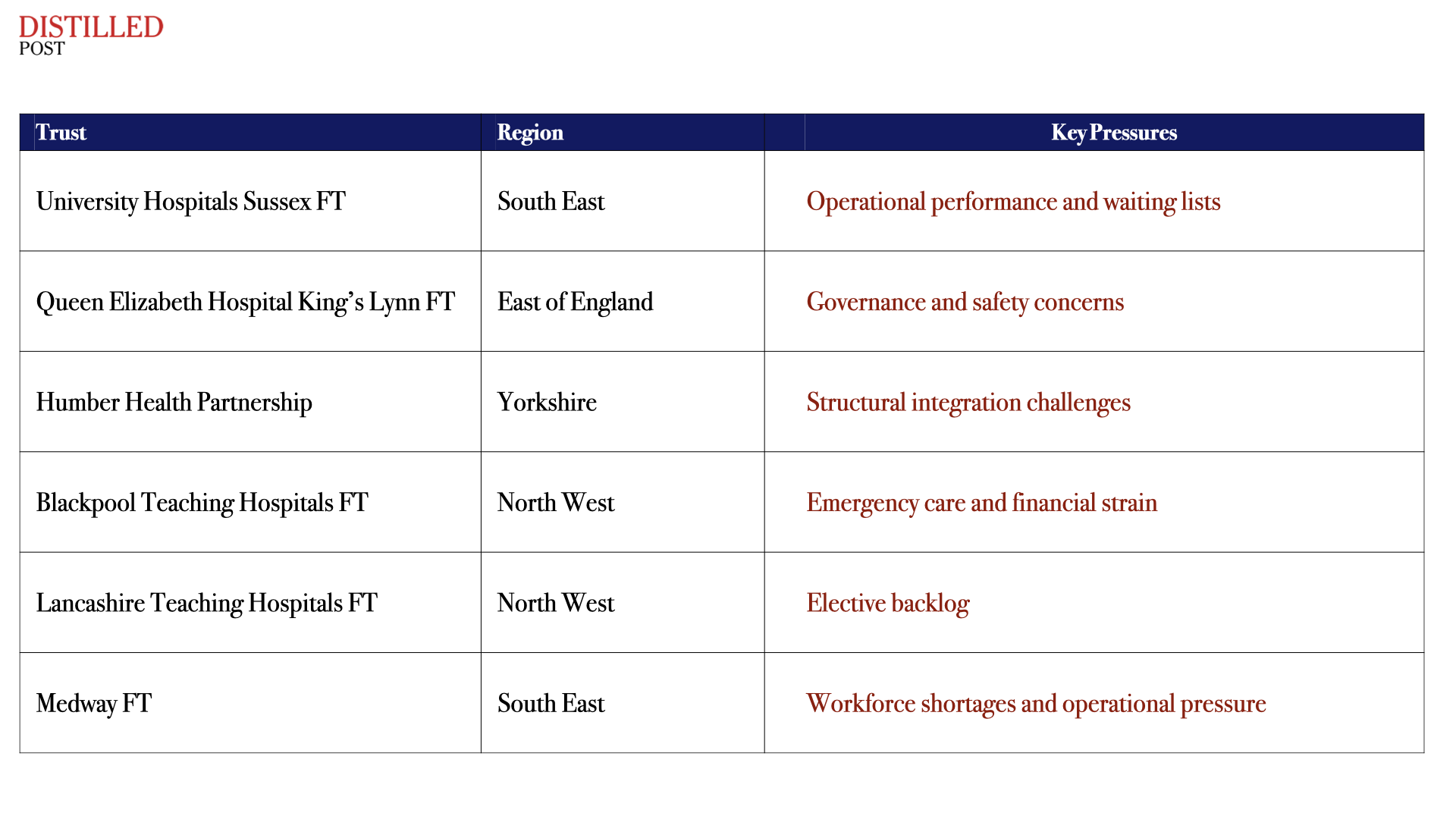
Nine trusts have been selected for the first wave of the programme. They represent a diverse group of organisations including large acute hospital providers, integrated regional partnerships and specialist mental health services. Several were already receiving support through earlier NHSE recovery regimes, suggesting previous improvement efforts have not delivered the scale of progress the national body expected.
The programme begins with an intensive diagnostic review led by NHSE improvement teams. The aim is to identify structural barriers preventing sustainable progress and to determine whether leadership teams have the capability and capacity to deliver recovery.
The launch of the programme reflects broader pressure building across the NHS. Hospitals continue to face record waiting lists, severe workforce shortages and financial deficits that are becoming increasingly difficult to contain. Many trusts have attempted internal reforms or partnerships with neighbouring organisations to stabilise performance, but in several regions improvement has remained fragile.
Inside NHSE there is growing recognition that some organisations are trapped in cycles of underperformance where incremental reforms cannot deliver lasting change. The new programme therefore introduces a more direct oversight model that combines operational support with the potential for structural intervention if improvement fails to materialise.
Over the coming months NHSE will work closely with leadership teams inside the selected trusts to develop detailed recovery plans. These plans will outline operational gaps, set measurable milestones and define the pace at which improvement must occur. The findings will then inform NHSE decisions about whether further regulatory action is required.
For trust executives the programme effectively becomes a test of organisational credibility. If leadership teams can demonstrate clear progress and deliver realistic recovery plans, the programme may act as a stabilising force. If not, NHSE retains the ability to escalate intervention through governance changes, service reconfiguration or deeper system level restructuring.
The significance of the initiative extends well beyond the nine trusts currently involved. It signals a shift in how NHSE intends to manage institutional failure across the health service. For years improvement regimes often stretched over long periods without resolving structural weaknesses. The new model suggests a willingness from the centre to move faster when progress stalls.
That change reflects the scale of pressure now facing the NHS. Demand continues to rise, workforce capacity remains constrained and financial headroom is limited. In that environment persistent operational failure is no longer treated as a local management issue but as a systemic risk that national leaders must address.
For the nine organisations now under NHSE oversight the coming months will determine whether the programme becomes a platform for recovery or the first step toward more dramatic intervention. Either outcome will shape how the health service manages struggling providers in the years ahead.




.png)
.png)
.png)
.png)