

The argument over the NHS Federated Data Platform has moved beyond technical detail into something more fundamental. It is now a question of direction. Whether the NHS continues to build a connected, data-driven operating model, or retreats into a system defined by local optimisation and national fragmentation.
Calls to cancel the contract with Palantir Technologies have brought that choice into sharp focus. The concerns driving those calls are familiar. Questions of vendor history. Data sovereignty. Transparency. The risk of long-term dependency. These are not trivial issues, and they deserve scrutiny.
But they now sit alongside a growing body of operational evidence that is far more concrete. Across hospitals in England, the platform is already delivering measurable improvements in how care is managed, prioritised and delivered.
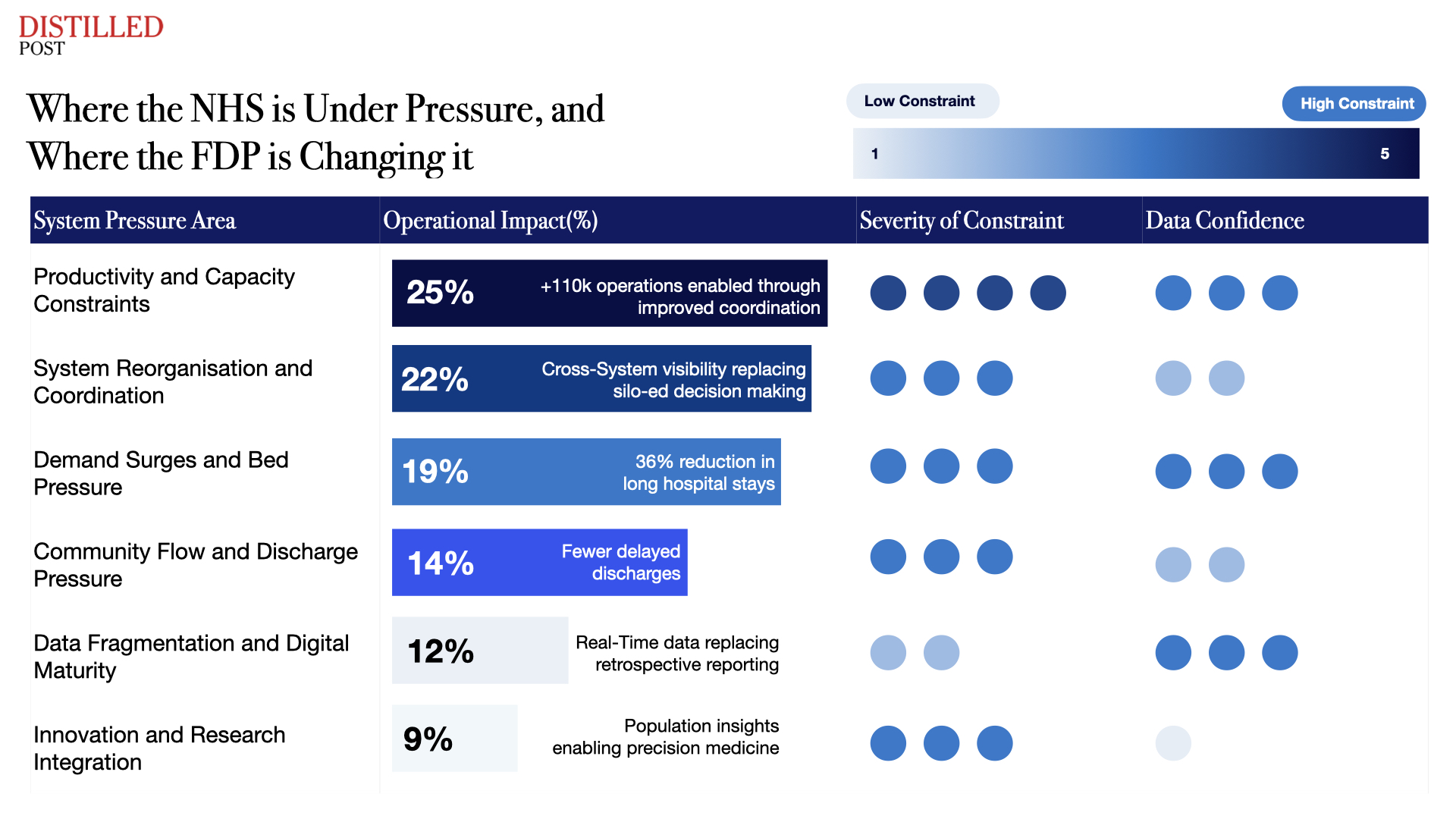
At a national level, the impact is clear. More than 110,000 additional operations have been delivered since the platform’s introduction. Waiting times for cancer diagnostics have fallen by 6.8 per cent. Over 123 NHS trusts are now using the platform, with the majority reporting tangible benefits in day-to-day operations.
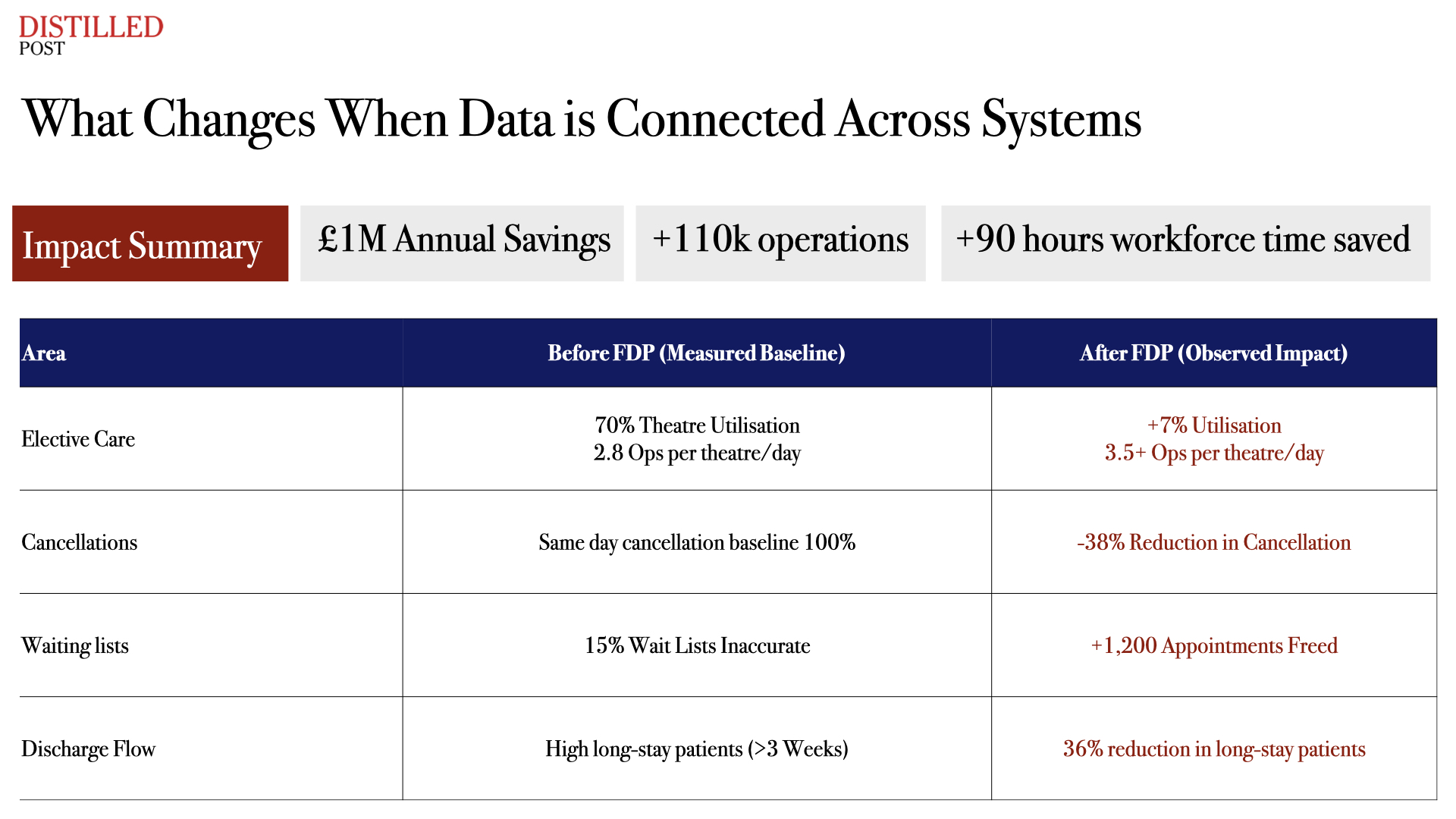
The efficiency argument is often the starting point for supporters of the platform. By connecting previously siloed systems, the FDP allows hospitals to manage waiting lists, theatre capacity and discharge pathways with far greater visibility. That, in turn, reduces delays and increases throughput.
Critics counter that many trusts already operate advanced local systems, tailored to their specific needs. There is a concern that a national platform risks overriding solutions that already work.
But this framing misses the scale of the problem. The NHS does not operate as a collection of isolated organisations. Patients move across trusts, services and care settings. Fragmentation between systems creates friction at those boundaries, where coordination is most critical. Local optimisation cannot resolve system-wide inefficiency.
The FDP addresses that gap. It sits above existing systems, connecting them rather than replacing them. Its value lies in enabling coordination across organisational lines, something local solutions were never designed to achieve.
Security concerns have also featured prominently in the debate. The use of Privacy Enhancing Technology ensures that data remains under NHS control, with access governed by strict permissions. The platform processes data under instruction. It does not own, sell or commercialise it. Fears of “mission creep” reflect broader anxieties about how data could be used beyond healthcare. Within the NHS, however, the application is tightly bounded. The system supports operational management, clinical prioritisation and service coordination. Its function is defined by those use cases.
Transparency has been another point of contention. Critics argue that success claims rely on internal reporting and that elements of the contract remain redacted. Scrutiny in this area is appropriate. But operational improvements observed within trusts provide an independent layer of evidence. Reduced cancellations, improved theatre utilisation and faster discharge processes are measurable within services themselves.
The question of vendor choice has also been challenged. Some argue that early involvement during the pandemic created an uneven playing field. What followed, however, was a formal procurement process designed to test technical capability, scalability and financial resilience. Delivering infrastructure at NHS scale requires a level of investment and engineering capacity that is limited to a small number of providers globally.
This leads to the concern around lock-in. The underlying software is proprietary, and switching providers would carry cost. That is a characteristic of most large-scale digital systems, across both public and private sectors. The relevant question is whether the system delivers sufficient value to justify its continuation.
On that measure, the evidence continues to accumulate. Beyond operational performance, the platform is beginning to enable advances in clinical research. For complex specialties such as oncology, the ability to analyse data across populations rather than individual institutions represents a significant shift.
As Dame Cally Palmer of the Royal Marsden NHS FT has argued, federated data systems allow for population-level insights that individual hospital systems cannot generate. In cancer care, this opens the possibility of identifying patterns in diagnosis, treatment response and outcomes at scale, supporting more precise and personalised approaches to care. This research dimension extends the value of the platform beyond immediate operational gains. It positions the NHS to generate insight as well as deliver care, linking service delivery with innovation.
Some critics argue that association with a controversial vendor could lead to increased patient opt-outs, reducing the completeness of the data and limiting the platform’s effectiveness. Of course, trust is fundamental. But it is also shaped by outcomes. Shorter waiting times, fewer cancellations and more coordinated care contribute to public confidence in the system. The relationship between data use and trust evolves as those outcomes become visible.
The NHS has spent decades attempting to modernise its digital infrastructure, often with limited success. The result has been a system defined by fragmentation, duplication and delayed decision-making. The Federated Data Platform represents a different approach. It builds on existing systems, connects them and applies data in real time to operational challenges.
The debate about whether to continue with that approach is ultimately a question of trade-offs. On one side sit concerns about governance, control and future risk. On the other sits a growing body of evidence showing improvements in how care is delivered today. Cancelling the contract would not return the NHS to a neutral position. It would return it to a fragmented one.
At a time when demand continues to rise, workforce capacity remains constrained and waiting lists dominate the political agenda, the cost of that reversal would be immediate. The NHS has reached a point where digital infrastructure is no longer optional. It is central to how the system functions. The evidence suggests that the Federated Data Platform is beginning to provide that foundation.
The question now is whether progress is sustained, or set aside.




.png)
.png)
.png)
.png)