

History tends to remember powerful technologies by their most extreme consequences. Nuclear fission transformed energy production, yet the atomic bomb dominates public memory. Advances in artificial intelligence promise productivity and insight, yet concern centres on surveillance and control. A pattern repeats. A technology emerges, its most controversial application captures attention, and everything that follows is judged through that lens.
The NHS Federated Data Platform has entered that same space. It now sits at the centre of one of the most politically charged debates in British healthcare. Questions about data governance, vendor history and public trust deserve serious attention. The NHS holds some of the most sensitive information in the country, and any system operating at national scale should be subject to scrutiny.
Yet the current conversation has narrowed. Focus sits heavily on who is involved and what they represent. Far less attention is given to what is happening inside hospitals as a result.
Meanwhile, the pressures facing the NHS continue without pause.
Inside hospital operations, the challenge has been consistent for years. Patients wait too long. Information moves too slowly. Staff work across fragmented systems and make decisions with only part of the picture in view. A clinician may need to check multiple platforms to understand a single patient journey. An operations team may lack a real-time view of theatre capacity across a trust. Discharge teams often coordinate across hospitals and local authorities without a shared view of who is ready to leave and what support is available.
These conditions define how care is delivered every day. They shape how quickly a patient is treated, how long they remain in hospital, and how effectively staff can do their jobs.
Fragmentation carries a cost. It delays treatment. It wastes capacity. It increases pressure on a workforce already under strain. The absence of connected data influences outcomes in ways that are often hidden but widely felt.
Over the past two years, that picture has begun to shift.
Tools built on the Federated Data Platform are now in use across a growing number of NHS trusts. They sit across existing systems, connecting data that was previously siloed and presenting it in a way that supports real-time decision making.
The effect is visible in day-to-day operations, and in places like Chelsea and Westminster Hospital, measurable at scale.
Across 8,637 theatre sessions spanning 14 specialties, analysis conducted with support from Imperial College London identified a 7 per cent improvement in booked utilisation when lists were planned and locked in advance. For those same sessions, where clinicians reviewed and confirmed lists at least two weeks ahead of surgery, day-of-surgery non-attendance dropped to zero. In a system where last-minute cancellations routinely waste clinical time, staff capacity and patient preparation, that change is significant.
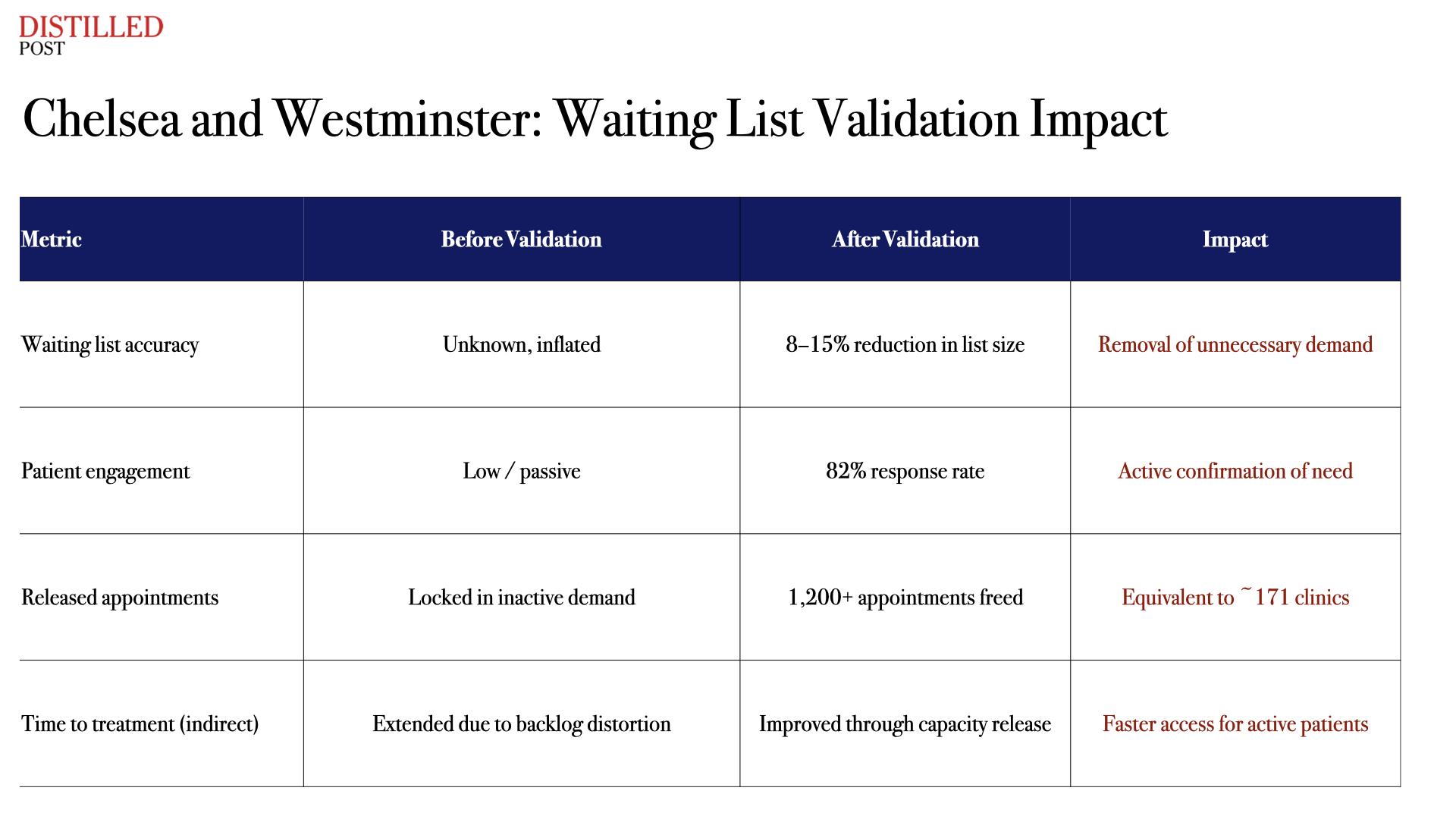
The impact extends beyond theatres. At ChelWest and across the wider North West London system, patient-led validation programmes have contacted thousands of patients on waiting lists, achieving response rates above 80 per cent. Between 8 and 15 per cent of patients were found no longer to require their scheduled care, releasing over 1,200 appointments back into the system. That equates to more than 170 clinics worth of capacity created without building a single new facility.
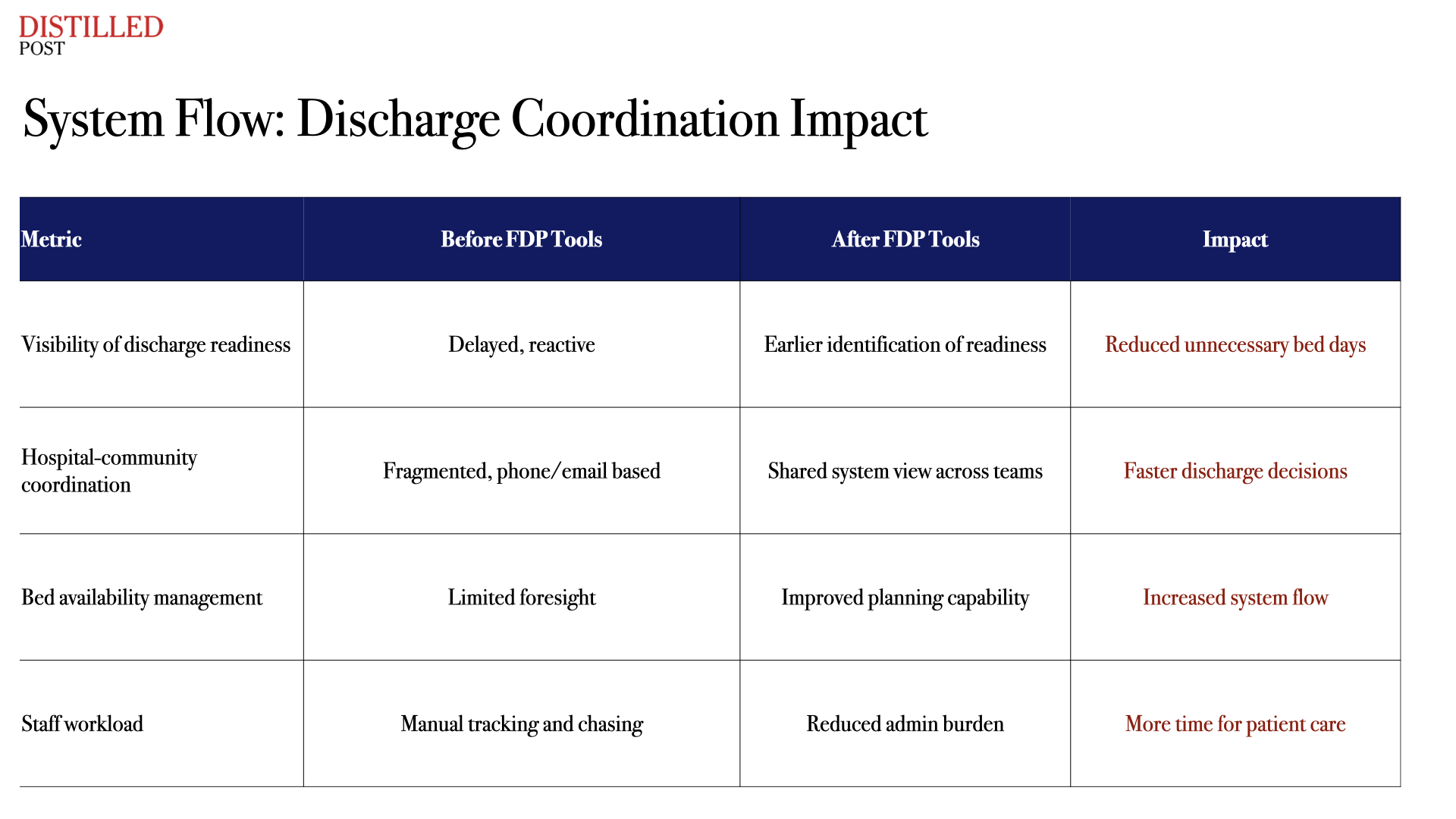
For discharge teams, similar improvements are emerging. Tools that allow staff to see, earlier in the pathway, when a patient is likely to be ready to leave hospital have begun to reduce unnecessary bed days. Coordination between hospital teams and local authorities has improved, with shared visibility replacing the need for repeated calls and manual tracking.
At a national level, the cumulative effect of these changes is becoming visible. For staff, this has meant less time spent navigating multiple systems. Fewer manual workarounds. Greater confidence in the data in front of them. The ability to act earlier, with a clearer understanding of the full pathway. This context rarely breaks through into the public conversation.
The debate continues to revolve around ethics, politics and association. Those dimensions matter and should remain part of the discussion. Alongside them sits another question that carries equal weight. What happens when the NHS chooses not to use tools that improve how care is delivered?
The current operating model offers a clear answer. Fragmentation limits capacity and slows decisions. Delays follow. Staff compensate. Patients wait. Inside hospitals, that trade-off is not theoretical. It plays out in real time. A delayed discharge means a patient waiting in A&E for a bed. An unfilled theatre slot means another postponed operation. An outdated waiting list means patients who are ready to be treated continue to wait behind those who no longer need care.
Digital infrastructure within the NHS has often been treated as secondary. Programmes are piloted, evaluated and gradually adopted. Progress moves slowly. Systems remain disconnected. Other sectors have taken a different approach. Data connectivity has been treated as core infrastructure, underpinning how the entire system operates. The NHS now has the architecture to do the same. Systems can be connected. Data can be used in real time. Evidence of operational impact continues to grow.
What follows depends on how that capability is used. Inside hospitals, the focus remains practical. Reducing waiting times. Using existing capacity more effectively. Giving staff the tools to manage complex care pathways with clarity. Patients experience the NHS in even simpler terms. Time waiting for an appointment. Time spent in a hospital bed. Time between diagnosis and treatment. Better use of data reduces that time. Poor visibility extends it.
The NHS should continue to face scrutiny. Its partners should be held to account. Transparency and governance remain essential. The conversation also needs to stay grounded in outcomes.
The central question concerns performance. Whether these systems improve care in measurable ways.
Across hospitals in England, the evidence is building.




.png)
.png)
.png)
.png)