
For England’s hospital chief executives, the warning light is no longer flickering. It is flashing red. NHS England has withheld £454.9 million in deficit support funding from 13 integrated care systems in the final quarter of 2025–26. What was once a stabilising mechanism has become conditional, performance-linked and, for many systems, suddenly uncertain. The financial compact between centre and system is being rewritten in real time.
At the heart of this decision sits NHS England’s chief finance officer, Elizabeth O’Mahony, appointed to lead strategic and operational finance at a moment of acute fiscal pressure. The policy shift is deliberate. Deficit support funding, historically agreed at the start of the year to help systems reach breakeven, is now contingent on in-year financial performance. Thirteen systems have seen support paused following month-nine reviews. The total withheld has surged from £260 million at quarter three to nearly £455 million by year end. This is not a technical adjustment. It is a structural tightening of liquidity across some of the most financially exposed systems in the country. For hospital CEOs managing workforce gaps, record demand and fragile capital estates, the change introduces volatility where predictability once existed.
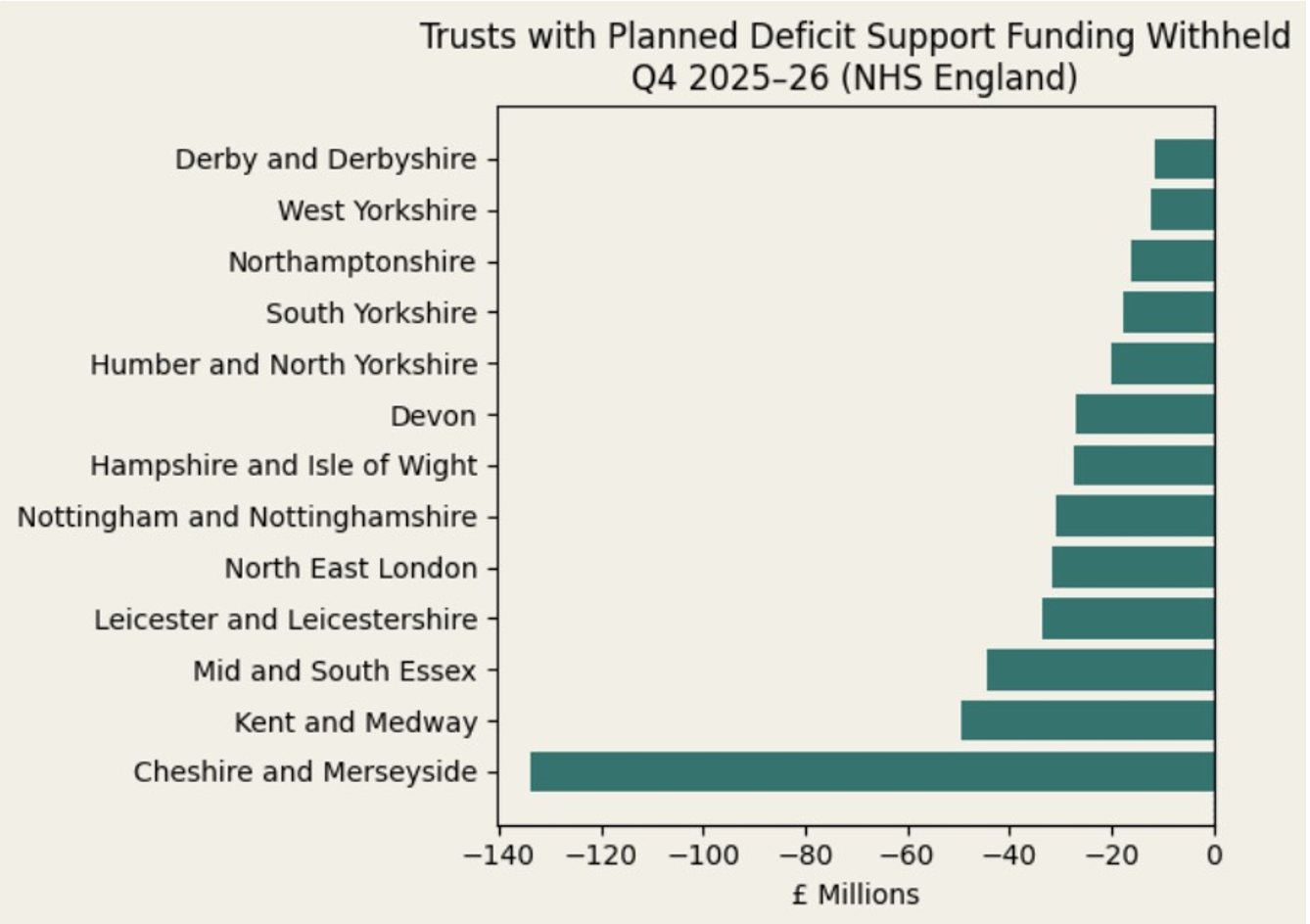
The distribution of withheld support underscores the scale. Cheshire and Merseyside alone accounts for £133.7 million, representing 2.1 percent of its core allocation. Kent and Medway has £49.3 million withheld. Mid and South Essex faces £44.4 million. Leicester and Leicestershire stands at £33.5 million. North East London has £31.5 million paused. Nottingham and Nottinghamshire £30.7 million. Hampshire and Isle of Wight £27.3 million. Devon £27 million. Humber and North Yorkshire £20 million. South Yorkshire £17.8 million. Northamptonshire £16.2 million. West Yorkshire £12.3 million. Derby and Derbyshire £11.3 million. In total, almost half a billion pounds has been effectively frozen pending remedial action. In percentage terms, the average withheld across affected systems is approximately 1 percent of core allocation. In operational terms, 1 percent determines whether theatre lists expand or contract, whether agency caps hold or break, whether digital transformation projects proceed or pause.
For chief executives, this is not about accounting optics. It is about cash flow resilience, covenant confidence and board assurance. Deficit support was designed to bridge structural gaps where local breakeven was not considered feasible. Withholding that support does not remove structural pressure. It shifts it downstream to providers.
This is where the strategic risk deepens. Elizabeth O’Mahony should be concerned not only about overspend trajectories, but about the unintended consequences of conditional support at scale. The NHS reported a £445 million year-to-date overspend at month nine. That gap is not cyclical noise. It reflects persistent demand, workforce cost inflation and residual pandemic impact. If overspending is structural, then suspending balancing funding in quarter four forces short term suppression rather than sustainable reform.
In practice, systems respond with recruitment freezes, delayed capital refresh, curtailed transformation programmes and tightened procurement. Those actions may produce headline improvement in-year. They do not fix underlying demand growth, ageing estates or workforce shortages. The danger for the national finance function is achieving control totals while eroding capability.
For O’Mahony, four strategic concerns should dominate.
First, liquidity instability. When funding becomes contingent late in the financial cycle, CFOs across trusts are forced into defensive cash management. Payroll, supplier confidence and investment planning all rely on predictable flows. Volatility undermines trust in the financial framework itself.
Second, structural misalignment. If systems are structurally underfunded relative to demand and cost base, performance-linked withholding risks penalising reality rather than inefficiency. Finance discipline is essential. But discipline without structural recalibration creates circular deficits.
Third, behavioural regression. Integrated care systems were created to encourage collaboration across providers. Conditional funding risks driving protective behaviour, as organisations shield their own positions rather than collectively redesigning care pathways.
Fourth, international divergence. While England constrains and conditions, peer health systems are investing forward. Scandinavian regions are embedding predictive analytics into operational command centres. Leading US integrated delivery networks are scaling AI-enabled scheduling and digital capacity modelling. Singapore continues to expand digitally enabled community infrastructure. Capital flows to innovation environments, not austerity cycles. If England’s financial regime prioritises short term balance over long term competitiveness, the performance gap will widen.
For hospital chief executives, the implications are immediate. Cash modelling becomes more granular. Scenario planning must assume delayed or partial support. Boards will need enhanced assurance frameworks to address going-concern questions. Investment committees may defer non-essential capital, even where long term returns are clear. Digital transformation programmes, often the first to pause in fiscal tightening, risk slowing just as productivity demands acceleration.
The narrative externally may frame this as fiscal rigour. Internally, it feels closer to enforced stress testing. Systems can technically earn back withheld support through remedial action. Providers may apply for emergency cash if needed. Yet that language itself signals fragility. Emergency funding is not a substitute for stable architecture.
The broader concern is reputational. The NHS remains a global symbol of universal healthcare. But sustained cycles of deficit normalisation followed by punitive tightening erode strategic credibility. Investors, technology partners and clinical talent observe patterns. Systems that appear locked in annual firefighting attract less innovation capital.
None of this diminishes the complexity facing NHS England’s finance leadership. Balancing a £170 billion system amid inflationary pressure and political scrutiny is formidable. But the path chosen matters. Conditional support must be accompanied by structural redesign, not solely compliance enforcement. Without parallel investment in productivity, digital capability and service redesign, the model risks compressing ambition.
For Elizabeth O’Mahony, the challenge is not simply closing a £445 million gap. It is preventing a financial control strategy from becoming a brake on transformation. For hospital CEOs, the task is equally stark: maintain operational resilience while arguing, with evidence and discipline, for funding frameworks that enable reform rather than episodic containment.
The £460 million withheld this year is more than a balance sheet adjustment. It is a signal about the direction of travel. If England’s health service continues to tighten inward while global counterparts invest outward, the consequences will not be immediate collapse. They will be gradual erosion. And gradual erosion, in complex systems, is often the most dangerous trajectory of all.




.png)
.png)
.png)
.png)