

In the spring of 2023, a row broke out across NHS corridors and Whitehall offices that rarely makes front pages. The question at its centre was deceptively simple: who does the data belong to, and who does it serve? It was, in miniature, the same question that has defined Andy Burnham's political career. Not data specifically, but the principle underneath it: whether public services are designed around the institutions that run them or the communities they are supposed to serve. Burnham has spent the better part of two decades arguing that the answer from Whitehall has too often been the former. A premiership would be his opportunity to test whether that can change at national scale.
Whether nine years as Mayor of Greater Manchester has actually proven the case is a more complicated question than his supporters tend to acknowledge.
The Manchester record is genuinely mixed. A major study commissioned by the Health Foundation and published in The Lancet Public Health found that life expectancy did improve in Greater Manchester during the devolution period compared with a synthetic control group drawn from similar areas of England. But there were also increases in adult obesity and higher waiting times for treatment in A&E. The researchers themselves were cautious about attribution: the study tells us that life expectancy improved in Greater Manchester during the period of devolution, but cannot tell us how far these improvements were driven by health and social care devolution, devolution of wider public services, or some other longer-run changes in the region. That ambiguity matters. Burnham governed for nine years, the equivalent of two full parliamentary terms. The improvements are real but modest, and the causal chain between his mayoralty and the outcomes is contested by the researchers who examined it most carefully.
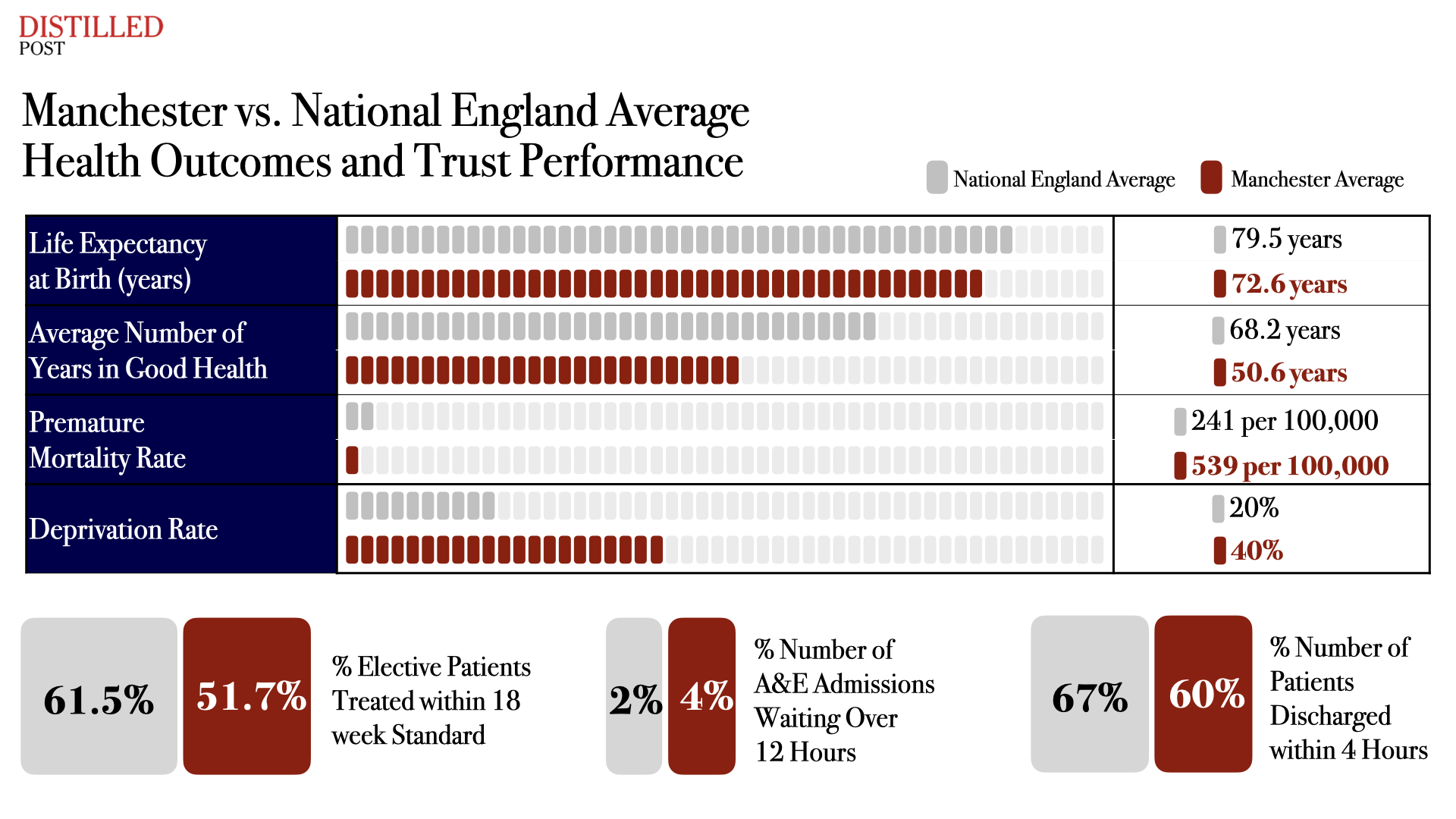
The structural context is also important. Healthy life expectancy at birth for males in Greater Manchester improved to 61.68 years, still remaining below the national average. For females it was 60.83 years. Premature mortality rates in Manchester sit at 539 deaths per 100,000 population, compared to 241 per 100,000 in Kensington and Chelsea. A baby boy born in Manchester can expect to live 17 fewer years in good health than a baby boy born in Richmond upon Thames. These are not gaps that opened on Burnham's watch, and it would be unfair to hold him responsible for decades of structural deprivation. But they have not closed substantially during his tenure either, and the honest account of Greater Manchester's health trajectory is of incremental improvement against a very high base of need, not a system that has been visibly transformed. Following devolution, primary care practices in Greater Manchester remained reliant on funding from national funding schemes that poorly reflected its deprivation, and the devolved administration's ability to address health inequities at the primary care level appeared uncertain.
The early years of health and social care devolution in Greater Manchester, according to qualitative evidence, involved time-consuming work to build relationships, establish governance, and develop new strategies and plans, but changes in services likely took longer to deliver. A national government does not have the luxury of that kind of runway.
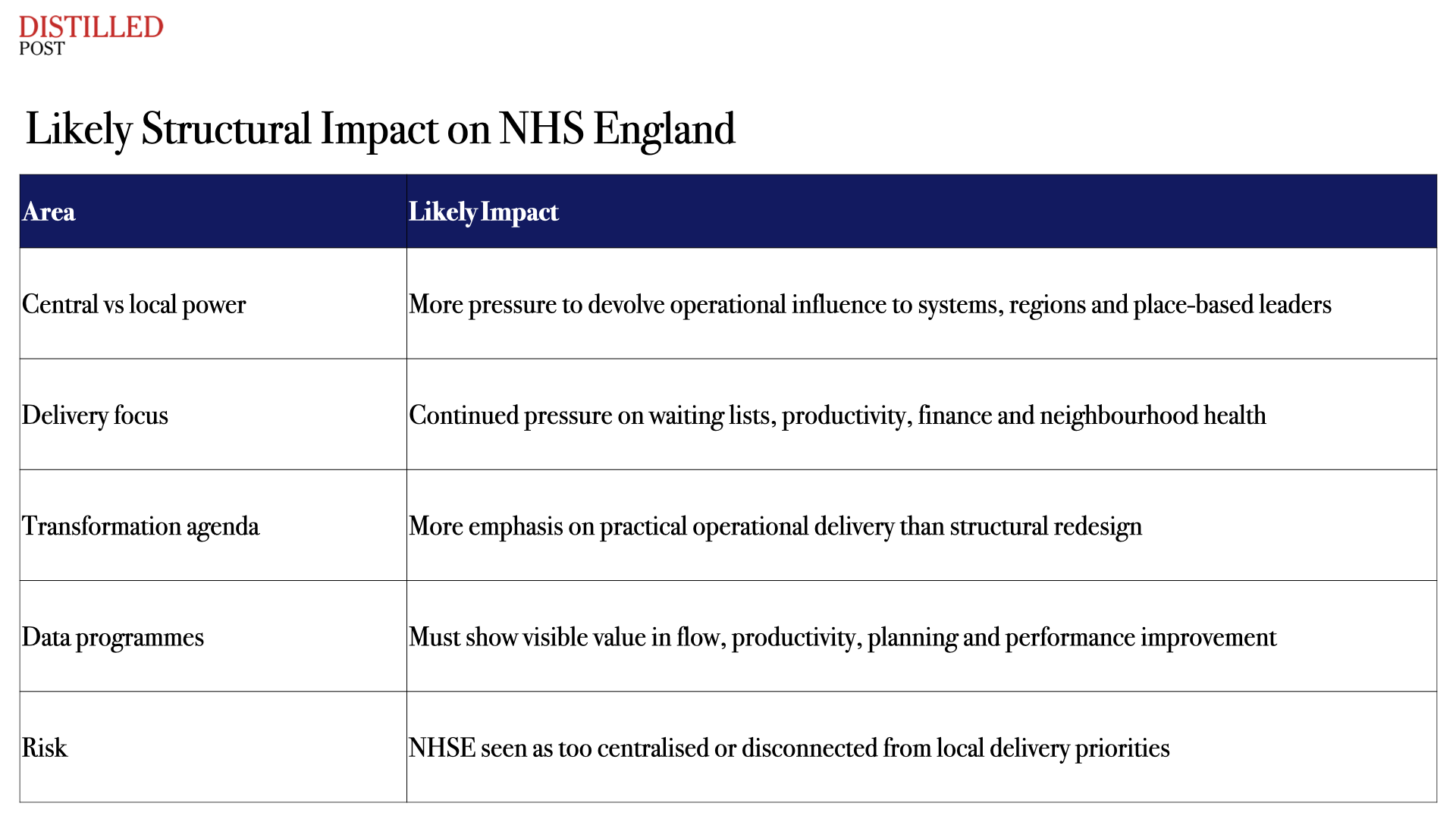
Burnham would arrive in Downing Street with a delivery agenda rather than a reform agenda. There will be no appetite for top-down reorganisation. The pressure on NHS England to cede operational influence to Integrated Care Boards, regional trusts, and place-based leaders would be significant. The expected cabinet alignment supports this direction: James Purnell as Chief of Staff brings deep familiarity with public service delivery, and Wes Streeting at Health and Social Care has already moved in Burnham's direction. In a major speech in March this year, Streeting explicitly credited Burnham's influence in shaping new health devolution deals for Greater Manchester and South Yorkshire, with ICB chairs effectively becoming deputy mayors for health. Streeting described it as the most radical reform in NHS history. That may be so. Whether it works outside Manchester's specific political and governance conditions remains to be established.
The challenge Burnham faces is the same one that has defeated every reforming Health Secretary for thirty years: social care. In 2009, as Health and Social Care Secretary, he proposed a National Care Service for England, a unified system designed to end what his green paper called the "cruel lottery" of means-tested social care. A general election intervened before it could be legislated. No subsequent government found the political will to revive it. The Starmer government commissioned Baroness Casey to review social care in 2024, but that process is unlikely to produce legislation before the next election, squandering, as one observer noted, an opportunity to use a substantial parliamentary majority to deliver meaningful change. Burnham would arrive with sixteen years of accumulated intent on this question and, potentially, a fresh mandate to act. Whether the fiscal headroom exists to fund what genuine integration actually requires is a different matter.
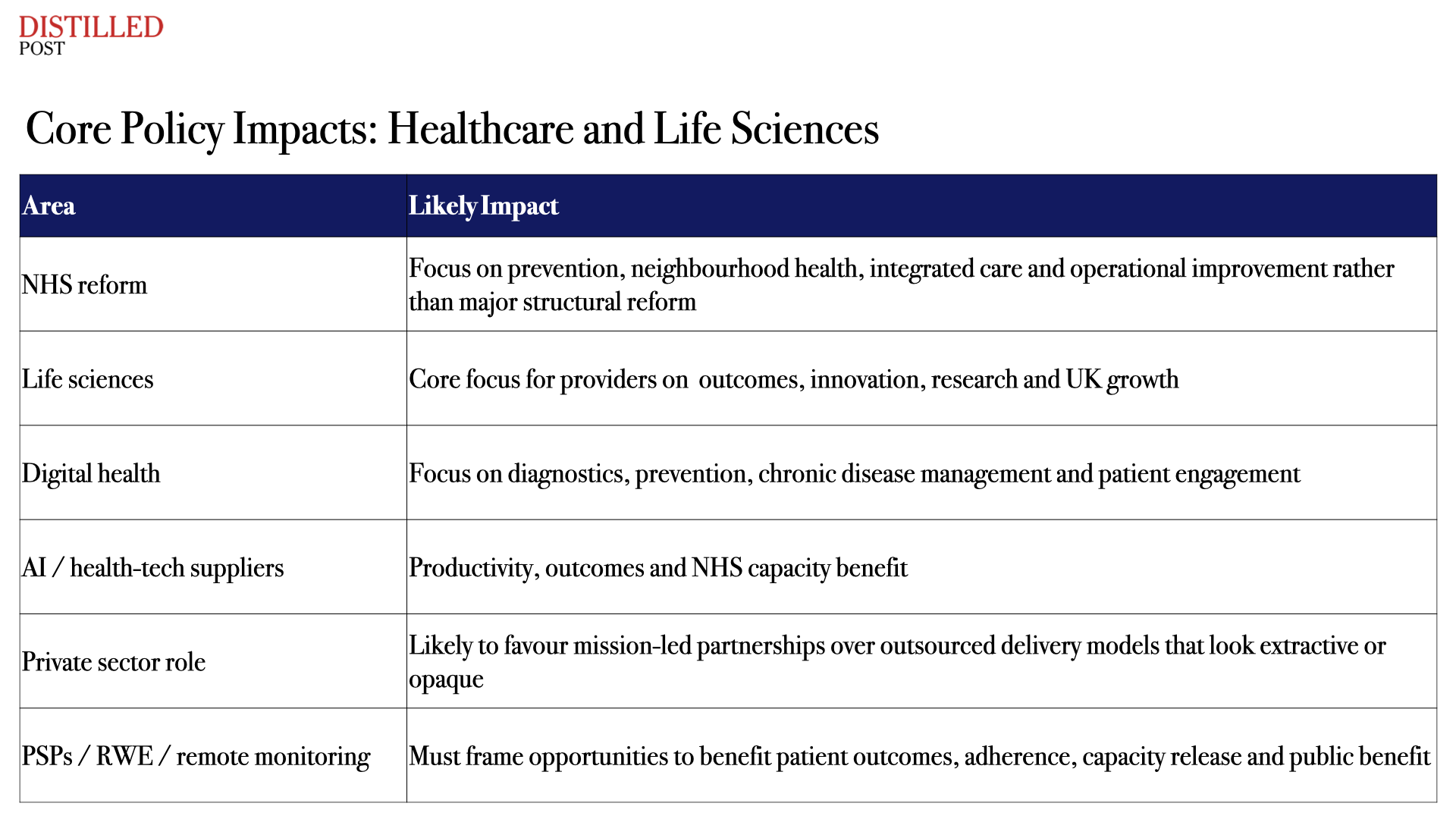
For private sector partners and life sciences companies, the Burnham era signals a shift away from the commercial models of the previous decade. Vendor-locked contracts, technology demonstrations that never scaled, and partnership agreements that prioritised supplier capability over measurable public benefit will face sharper scrutiny. Burnham's approach in Manchester was collegiate, drawing businesses in as partners rather than contracting at arm's length. There is no indication he would abandon Streeting's NHS Ten Year Plan, the Life Sciences Sector Plan, or the Value-Based Procurement methodology already in place. The continuity is real. What would change is the standard of accountability applied to whether those frameworks are actually delivering for patients.
The NHS the next government inherits is under profound pressure. The percentage of waits within 18 weeks ranged from 53% to 74% across integrated care boards, highlighting substantial geographical inequality underlying national performance, with the range between the highest and lowest median waiting times having more than doubled since 2019. That variation is itself an argument for place-based accountability. It is also a reminder that nine years of devolved governance in one of England's most politically coherent regions produced mixed health results, at a time when the challenges facing a national government trying to extend that model across forty-two integrated care systems, each with its own political dynamics and legacy pressures, will be an order of magnitude greater.
Burnham is a politician of genuine conviction with a specific and considered theory of how the NHS should change. That is rarer than it sounds. But conviction and a compelling theory of change are not the same as a proven model at national scale. The question his premiership would have to answer is whether what worked, partially, in Greater Manchester over nine years can be made to work across England in a parliamentary term, against a fiscal backdrop that offers little margin for error and a health system that has been told, repeatedly, that transformation is imminent.




.png)
.png)
.png)
