

The National Health Service does not lack operating theatres in the way it is often assumed. What it has lacked, until recently, is a clear and unified understanding of how those theatres are used.
For many years, the constraint on surgical capacity has been attributed primarily to workforce shortages, funding limitations and physical infrastructure. However, a growing body of evidence suggests that a more fundamental issue lies beneath these pressures. The way in which operating lists are constructed, coordinated and adjusted has historically been fragmented, opaque and inefficient. A recent study from Imperial College London, examining the NHS Federated Data Platform, offers one of the most detailed real-world analyses to date of how digital coordination can transform this dynamic.
At Chelsea and Westminster NHS Foundation Trust, the implementation of a centralised digital scheduling tool has resulted in measurable changes to how theatres are utilised. The findings provide a compelling illustration of how productivity gains can be achieved without expanding physical capacity.
A System Defined by Underutilisation
Operating theatres represent one of the most resource-intensive areas within secondary care, yet they have long been characterised by underuse. As recently as 2019, an estimated 38 per cent of theatre lists were not fully utilised, resulting in approximately £400 million of lost value each year.
The consequences of this inefficiency extend beyond financial waste. They contribute directly to prolonged waiting times, increased likelihood of same-day cancellations and deterioration in patient outcomes. By 2025, only 53.8 per cent of patients were receiving treatment within 18 weeks, significantly below the national target of 92 per cent.
These pressures are often interpreted as evidence of insufficient capacity. In reality, the system has frequently struggled to coordinate the capacity it already possesses.
The underlying causes of underutilisation are multifactorial, but they consistently point to fragmentation. Elective procedures must compete with emergency demand, scheduling information is dispersed across multiple systems and teams, and list construction often relies on manual processes with limited visibility. In such an environment, unused capacity is not always visible until it is too late to act upon it.
This fragmentation is not simply an operational issue. It reflects a deeper architectural challenge within the NHS’s digital estate, where systems have historically evolved in isolation rather than as part of an integrated whole. As Ming Tang has argued:
“The NHS must move away from bespoke standards and embrace internationally recognised ones to ensure interoperability across technologies. We need an environment where innovators, especially clinicians creating digital tools, can contribute easily. The pick and mix story for the NHS is how do we allow the technology stack to be much more plug and play so that different players can come and work with us.”
Her framing is critical. Without interoperability and a modular, plug-and-play architecture, the kind of real-time visibility required to optimise theatre usage cannot be sustained at scale. The challenge is not only to digitise processes, but to ensure that those digital systems can communicate, adapt and evolve together.
Reframing the Problem Through Digital Coordination
The introduction of the Federated Data Platform’s Care Coordination Solution represents a shift away from fragmented scheduling towards a more integrated and transparent approach. Rather than attempting to automate clinical decision-making, the system provides a single, shared view of theatre capacity across sites and specialties. This enables clinicians and schedulers to identify gaps, reallocate cases and optimise lists with a level of coordination that was previously difficult to achieve.
The effect of this change becomes evident when comparing operational performance before and after implementation.
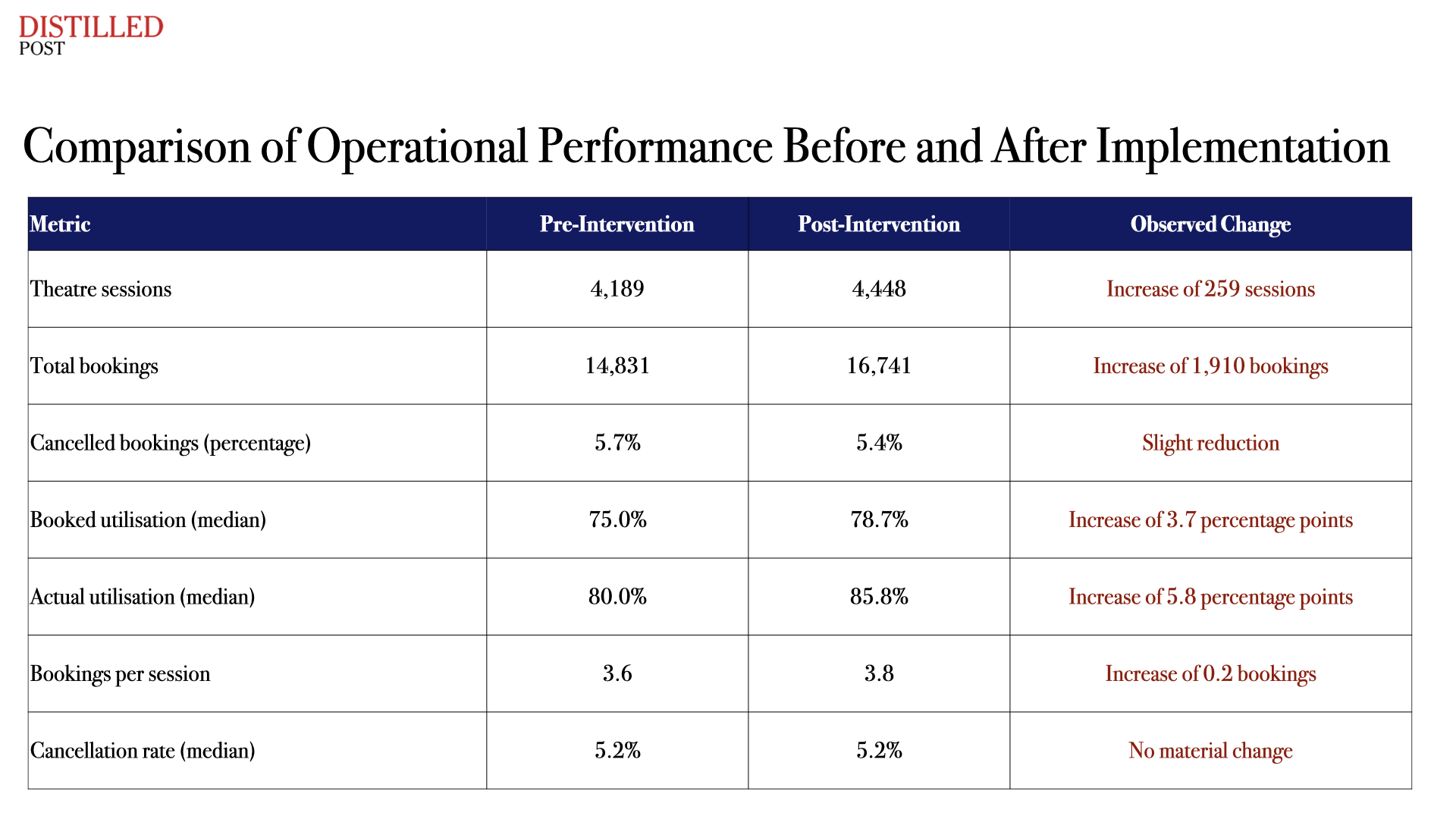
These figures indicate that, even without expanding infrastructure, the system was able to accommodate more activity and make more effective use of existing resources.
Divergence from the Expected Trajectory
The most significant insight from the study arises from the comparison between observed outcomes and a modelled counterfactual scenario in which the digital tool had not been introduced. Within six months, performance diverged meaningfully from what would otherwise have been expected.
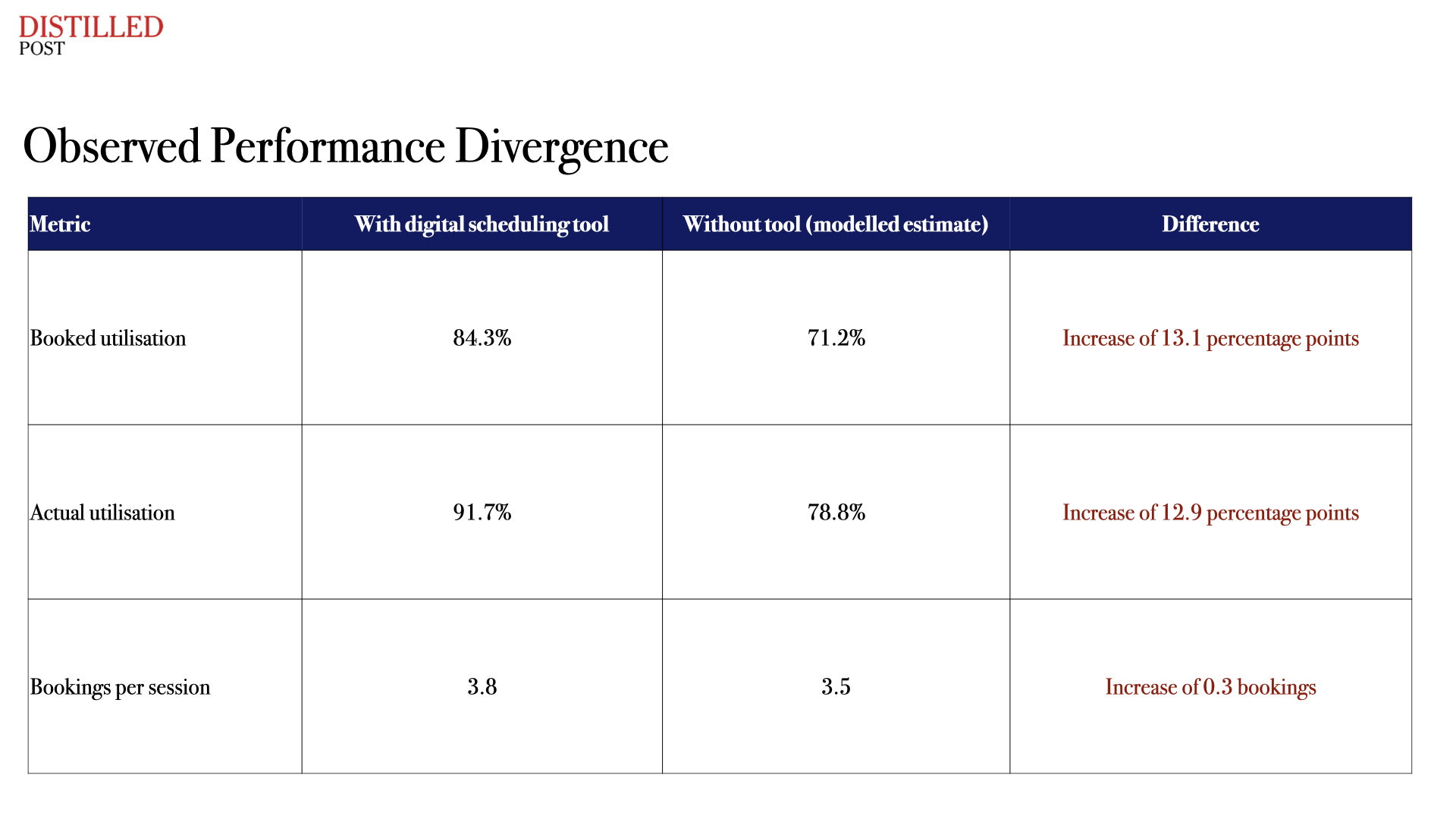
This comparison demonstrates that the improvements were not simply part of a broader recovery trend following the pandemic, but were associated with the introduction of the scheduling system itself. Across the full post-implementation period, these gains remained consistent and statistically robust.
The scale of these improvements is notable because they have traditionally been associated with substantial increases in capacity. In this case, they were achieved through improved coordination alone.
Evidence of Sustained Operational Change
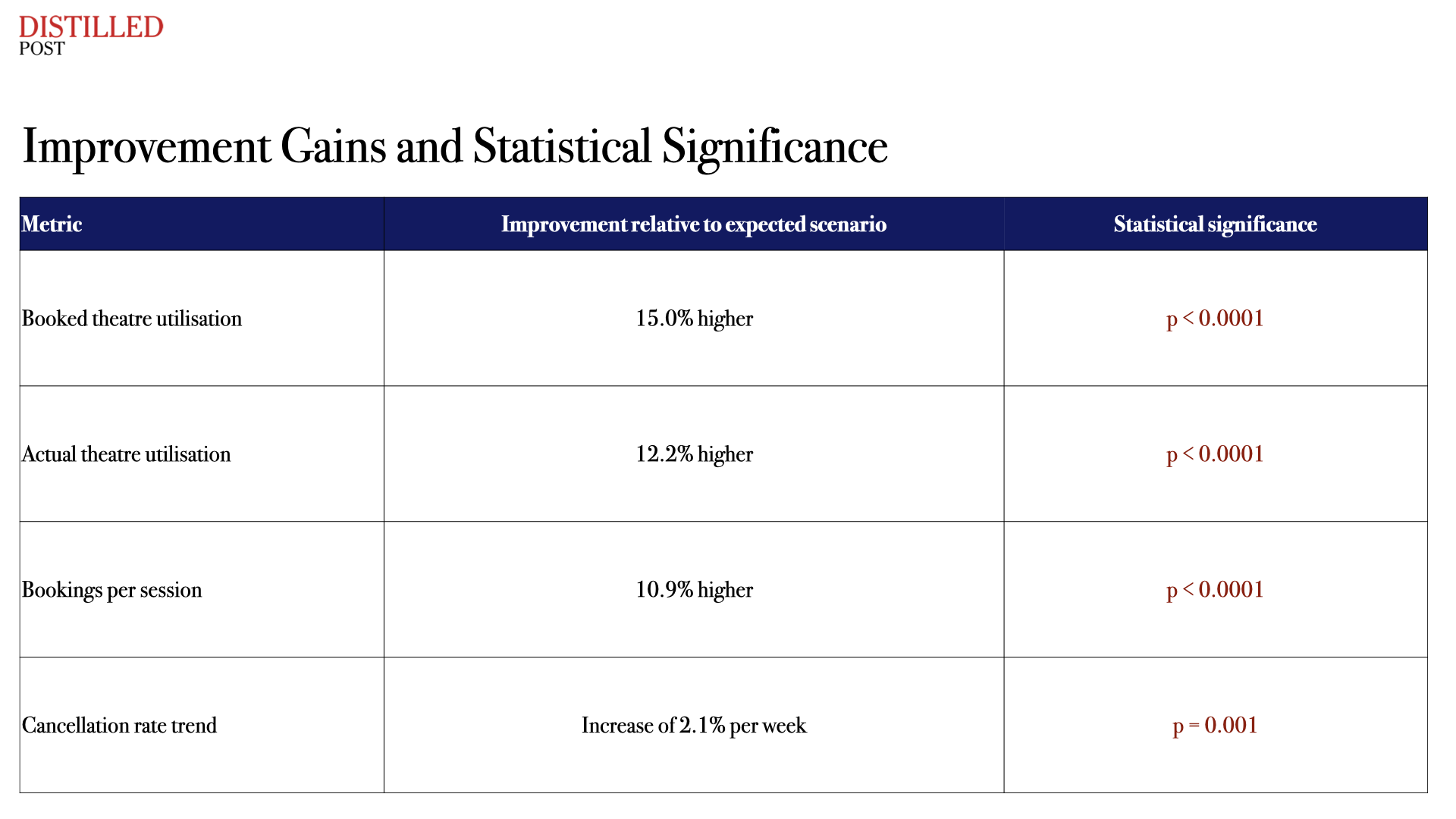
The statistical modelling used in the study provides further insight into how these improvements developed over time. The analysis identifies both immediate changes following implementation and ongoing trends that indicate sustained gains.
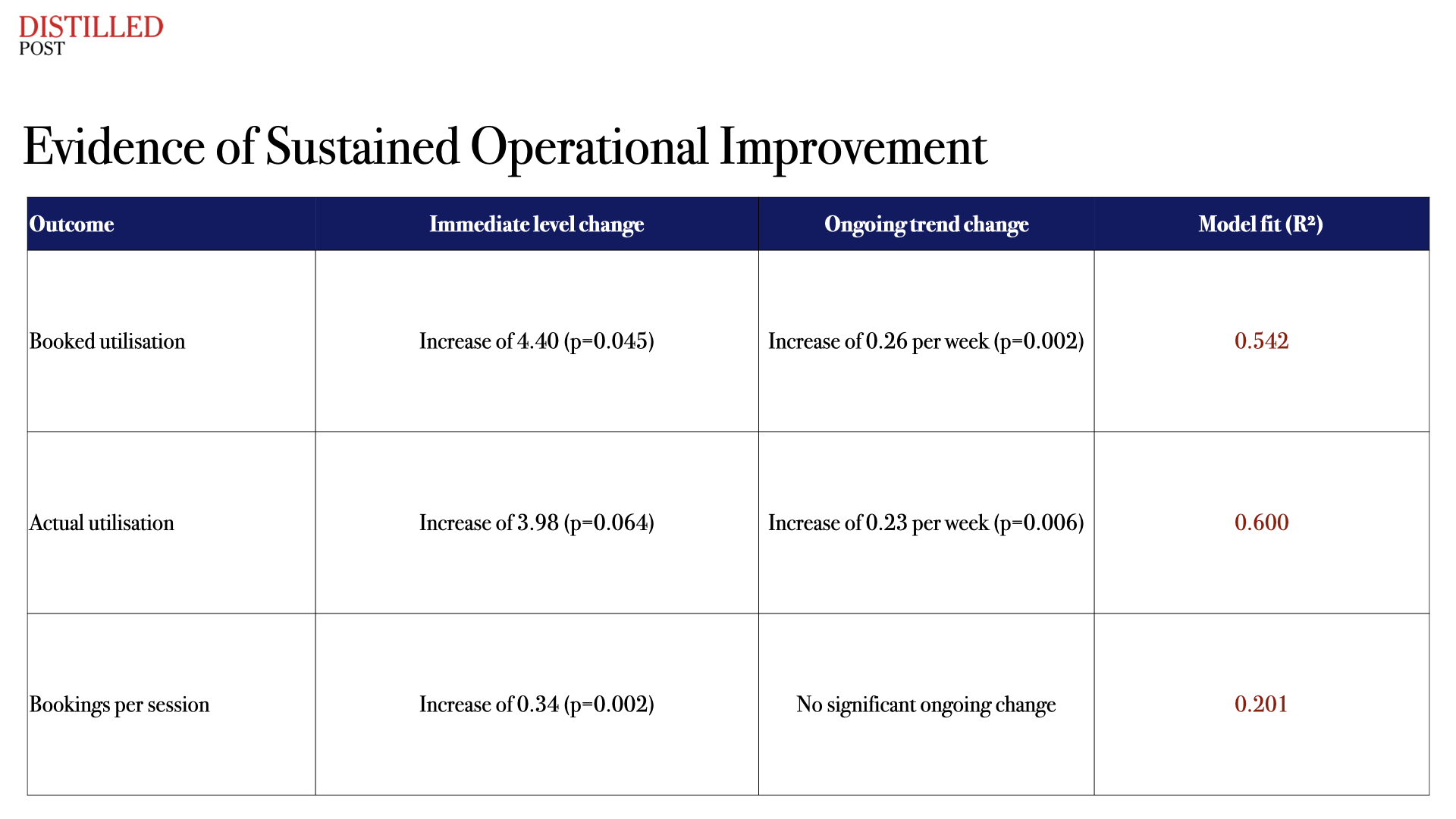
This pattern suggests that the intervention did not simply produce a one-off improvement, but altered the trajectory of performance over time. The system became progressively more efficient as it was used.
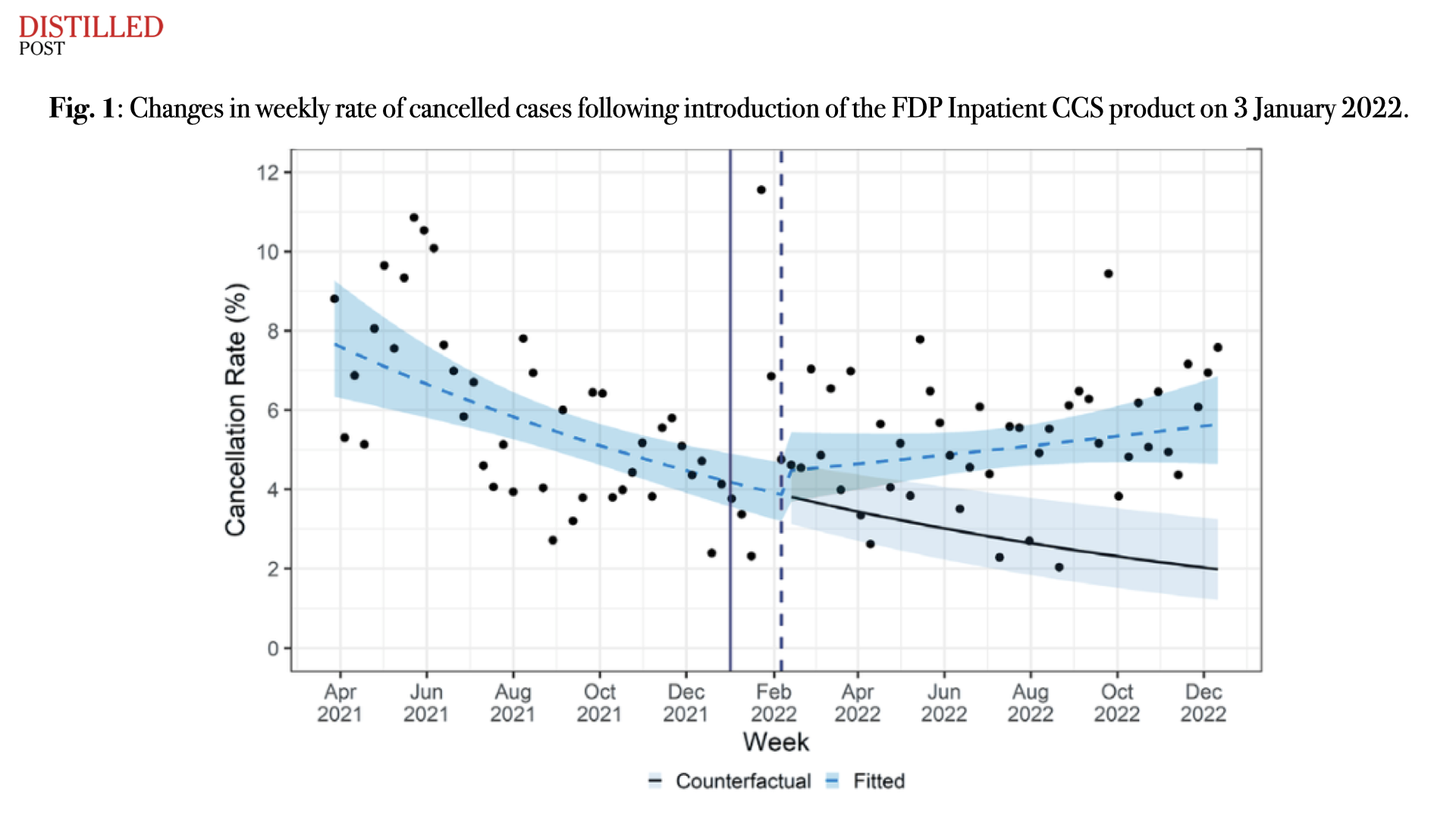
Interpreting the Increase in Cancellations
One of the more complex findings in the study relates to cancellation rates, which showed a modest upward trend following implementation. This might initially be interpreted as a negative outcome. However, the analysis indicates that median cancellation rates remained stable overall, and the observed increase may be linked to improved data visibility rather than deteriorating performance.
As scheduling processes become more transparent and easier to adjust, changes that might previously have gone unrecorded or been managed informally are more likely to be captured within the system. In this context, an apparent increase in cancellations may reflect a more accurate representation of operational reality.
From Capacity Expansion to System Coordination
The implications of these findings extend beyond theatre scheduling. They challenge a long-standing assumption that improvements in NHS performance must be driven primarily by increasing inputs such as workforce, funding or estate capacity.
Instead, they point towards a model in which productivity is achieved through coordination. When data from across the system is integrated and made accessible, decision-making becomes more informed and more collective. Lists can be adjusted dynamically, capacity can be redeployed where it is needed most, and inefficiencies that were previously hidden can be addressed in real time.
This represents a shift in how the system functions. It is not simply a matter of digitising existing processes, but of redesigning how those processes operate.
The NHS has often approached the challenge of waiting lists and elective recovery through the lens of expansion. More theatres, more staff and more funding have been seen as the primary solutions.
This study suggests that a different approach is possible. By improving visibility and coordination, it is possible to unlock capacity that already exists within the system and to use it more effectively.
The risk now lies not in a lack of technological capability, but in uneven adoption and incomplete implementation. If these tools are not embedded consistently across organisations and specialties, the potential gains will remain only partially realised.
What this evidence makes increasingly clear is that the NHS does not simply face a shortage of capacity. It faces a challenge of coordination.
The emergence of platforms such as the Federated Data Platform suggests that this challenge may now be addressable, provided the system is able to adopt and sustain the changes required.




.png)
.png)
.png)
.png)