

A forensic review shows one of the most demanding procurement processes in NHS history, where multiple global vendors competed and only one met the standard
The row over the NHS Federated Data Platform has generated more heat than light. But internal NHS England materials paint a different picture. Far from a rushed or politically driven decision, sources close to the matter describe a procurement process defined by depth, competition and scrutiny. Multiple global vendors entered, few survived. The real story is not that Palantir Technologies won. It is how rigorously everyone else lost.
At the centre of the process was the NHS England leadership team under Dame Amanda Pritchard, overseeing what insiders describe as one of the most complex digital procurements ever attempted in UK healthcare. This was not a standard tender. It was a full competitive dialogue model, designed specifically for programmes where requirements are too complex to define upfront. Suppliers entered early, but progression was unforgiving. Each stage required deeper technical validation, stronger operational proof, and tighter alignment to NHS delivery realities.
By the final stages, only three bidders remained. Earlier rounds had included major global technology providers, including hyperscalers and enterprise data firms, but the field narrowed quickly. The reason was simple. The NHS was not buying a tool. It was procuring national infrastructure.
The process itself was intensive. Over six weeks, 63 structured dialogue sessions were conducted with the final bidders. These were not presentations. They were working sessions, where suppliers were challenged line by line on architecture, delivery models, security assumptions and commercial structures. Feedback from participants described the process as unusually transparent and collaborative, but also demanding.
Crucially, bidders were required to build and demonstrate live platform scenarios. This was not theoretical compliance. It was real world validation. Suppliers had to prove that their systems could handle NHS scale data flows, integrate across fragmented systems, and deliver usable outputs for clinical and operational teams. Written responses alone were not enough. Capability had to be shown, not claimed.
The evaluation framework was equally rigorous. More than 30 subject matter experts from across the NHS were involved, spanning clinical, operational, digital and governance functions. Each evaluator assessed only their area of expertise, ensuring depth over breadth and reducing the risk of bias. No single individual had oversight of the full scoring process, a deliberate design to prevent influence.
Scoring was conducted independently, with each evaluator required to document their reasoning before entering moderation. Only after this were scores discussed and aligned. Mandatory training reinforced fairness, openness and impartiality, consistent with Cabinet Office standards. This was a controlled system, not an informal judgement.
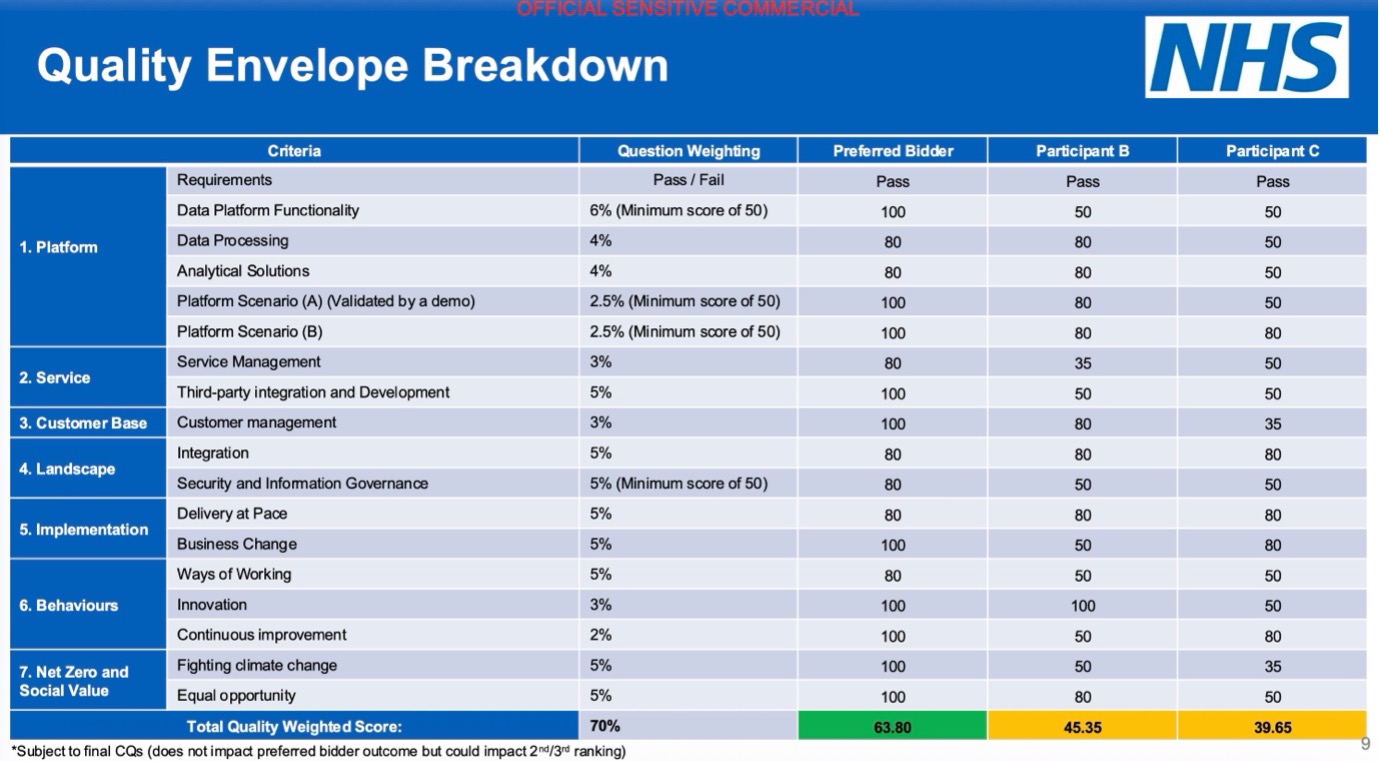
Quality carried the majority weight at 70 percent, with commercial considerations accounting for 30 percent. This matters. It meant the process prioritised capability, delivery confidence and long term value over short term cost. Suppliers were not rewarded for being cheapest. They were rewarded for being credible at scale.
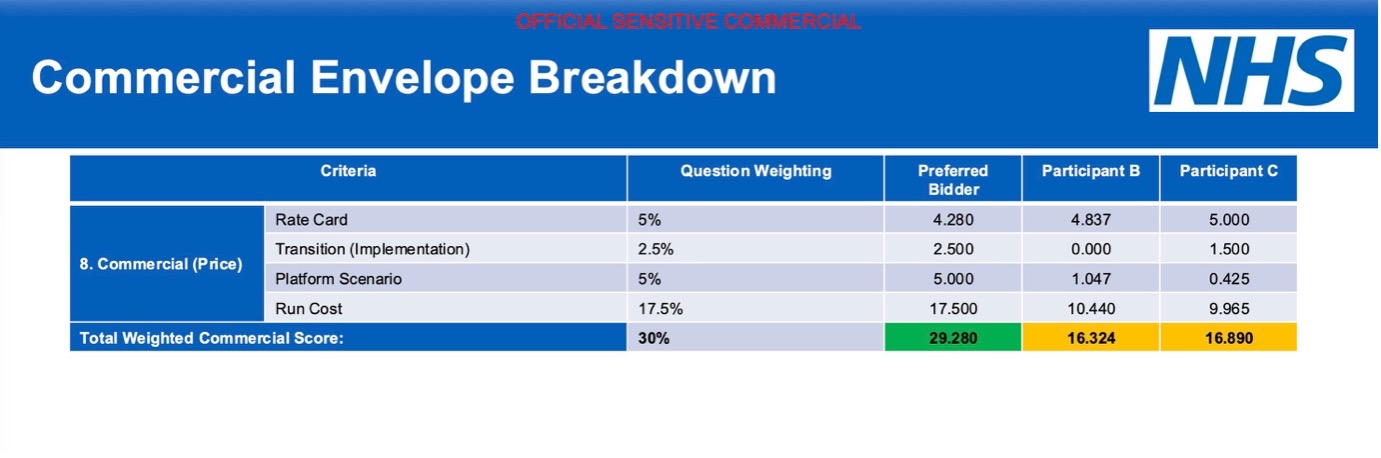
The commercial model itself was engineered to remove ambiguity. NHS England created a standardised pricing framework, forcing bidders into direct comparability. Weeks were spent reviewing cost assumptions in detail, ensuring that all participants priced against identical scenarios. Even abnormally low tender checks were applied to prevent unrealistic bids from distorting the outcome.
The result was not close. The preferred bidder outperformed competitors across both quality and commercial dimensions, with particularly strong performance in platform validation and delivery capability. This was not a marginal decision. It was a clear separation.
Our forensic review of the process points to one of the most demanding procurement exercises undertaken in the NHS in recent years. While sources were unwilling to speak on the record, those close to the matter were clear in their assessment. As one put it, “this is being driven by a small number of disgruntled individuals feeding sections of the press with misinformation, often linked to redundancies and the termination of service contracts within NHS England.”
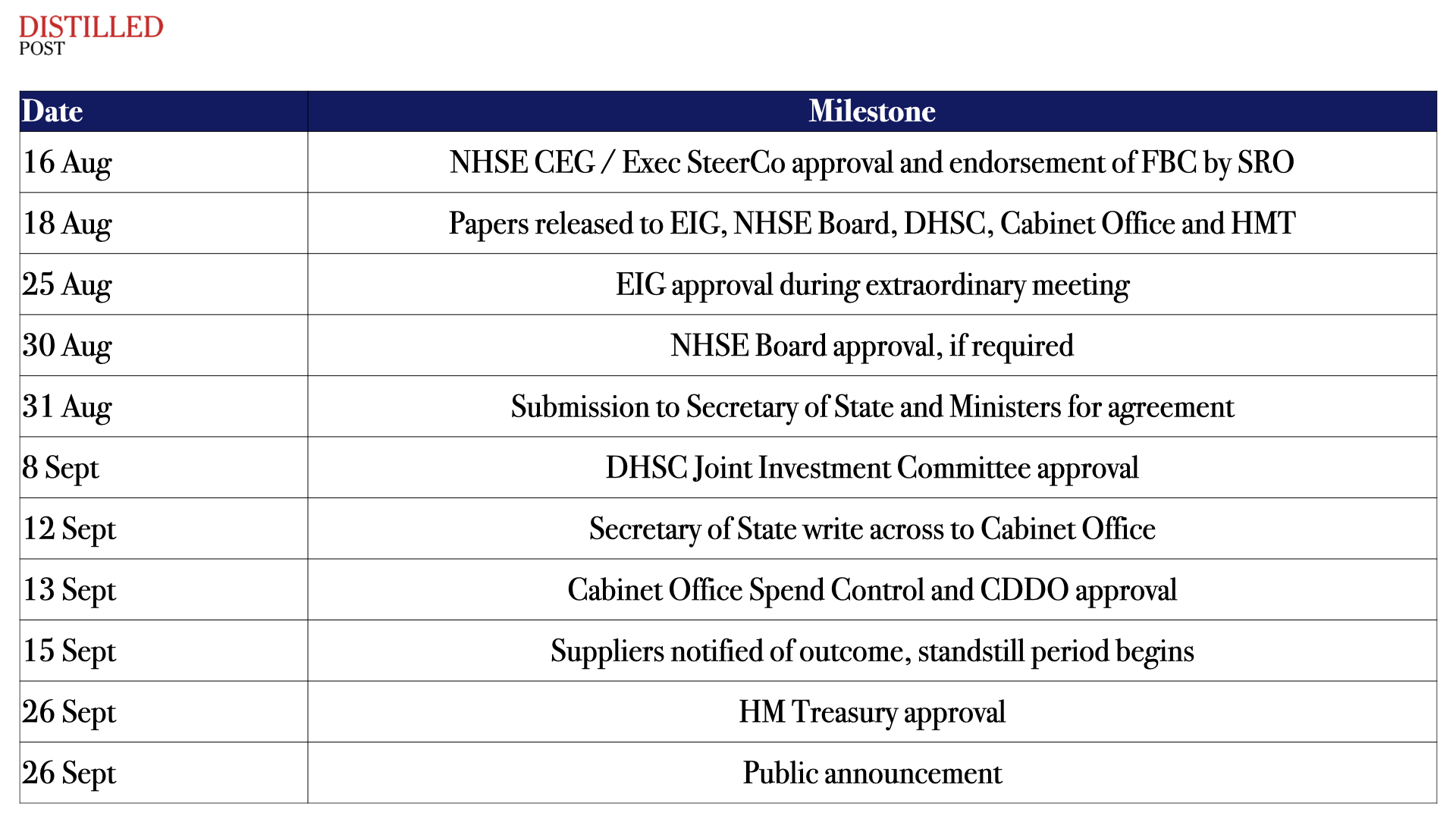
The structure of approvals itself reinforces just how tightly controlled the process was. The final business case moved through multiple layers of governance, each with its own scrutiny and sign off:
This is where the public debate often loses its footing. Much of the criticism has focused on Palantir’s broader work in defence, policing and government. Those concerns are not trivial. But they are also not the full picture.
Two things can be true at the same time. A platform can support national security operations and also underpin healthcare transformation. It can be used in policing and still reduce hospital admissions. It can operate in sensitive government environments and also help clinicians manage chronic disease more effectively.
The procurement process did not ignore these tensions. It embedded them into evaluation. Security and information governance were not peripheral. They were core scoring components with minimum thresholds. Fail to meet them, and you did not progress.
What the documents show is not a system captured by a single vendor, but one that tested multiple vendors and selected the only one that met the full requirement set. Several organisations could meet parts of the challenge. Few could meet all of it.
The real question now is not about the past. It is about what comes next. What assurances can Louis Mosley and his team provide that UK health data remains sovereign, isolated and protected? How is that demonstrated, not just stated?
Because trust in platforms like the FDP is not secured through procurement alone. It is built through delivery, transparency and governance over time. The NHS has made its choice based on capability. The next phase will determine whether that choice delivers the confidence, and the outcomes, the system now expects.




.png)
.png)
.png)
.png)